 |
|---|
|
 This issue of the Human Factors Quarterly focuses on advancing the practice of usability engineering of health IT (HIT) systems in VA. The first and second articles describe how VA clinicians have become ‘usability advocates’ for VA HIT systems. The third article outlines the role of the clinical informaticist in the usability engineering process. The fourth articleshowcases a new tool that enables HIT development teams gain a better understanding of the end users for whom they are designing. And the final article is a call to VA clinicians to support HIT usability by volunteering to be a usability study participant. As always, we welcome your feedback via e-mail to VHA10P2HFQ@va.gov. This issue of the Human Factors Quarterly focuses on advancing the practice of usability engineering of health IT (HIT) systems in VA. The first and second articles describe how VA clinicians have become ‘usability advocates’ for VA HIT systems. The third article outlines the role of the clinical informaticist in the usability engineering process. The fourth articleshowcases a new tool that enables HIT development teams gain a better understanding of the end users for whom they are designing. And the final article is a call to VA clinicians to support HIT usability by volunteering to be a usability study participant. As always, we welcome your feedback via e-mail to VHA10P2HFQ@va.gov.
From The Editor-in-Chief, Ross Speir
|
|
| |
 |
 |
An Interview with David Eibling, MD
Christopher Petteys, MBA, Project Coordinator, Human Factors Engineering (HFE), Office of Informatics and Analytics (OIA)
Dr. David Eibling is an otolaryngologist at VA Pittsburgh Healthcare System (VAPHS). He is also a distinguished Professor at the University of Pittsburgh’s Department of Otolaryngology where he shares his wisdom and knowledge with Ear, Nose and Throat (ENT) residents, medical students, and others. Dr. Eibling has a passion for patient safety and the discipline of Human Factors Engineering.
What is your role with VHA?...
Read More >
|
Upcoming Events:
Combined HSR&D/QUERI National Conference for Summer 2015, Location, TBD, Summer 2015
Designing Systems, Products and Services to Make them Easier, Safer, and More Effective for Human Use, Ann Arbor, MI, Jul 27 - Aug 1 and Aug 03-07, 2015
12th Annual International Naturalistic Decision Making Conference, McClean, VA, June 18-12, 2015
- Informational Links:
- Human Factors Engineering (HFE) within the Veterans Health Administration (VHA) Office of Informatics and Analytics, Health Informatics Division seeks to increase awareness of human factors products and services among clinical end-users and other stakeholder groups. This quarterly newsletter serves to engage these communities in shared communication and collaboration around human factors-related issues.
Access and review previous issues of this newsletter
- Editor-in-Chief:
- Ross Speir, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Managing Editor:
- Christopher Petteys, MBA, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Editorial Board Members:
- Michael W. Smith, PhD, Houston VA HSR&D Center for Innovations
- Rachel Wiebe, RD, CPHQ, Health Solutions Management, Health Informatics, Office of Informatics and Analytics
- Linda C Williams, RN, MSI, VA National Center for Patient Safety
- Scott D. Wood, PhD, Informatics Patient Safety, Office of Informatics and Analytics
|
 |
 |
Local Application and Transmission of User-Centered Design Principles
Tim Arnold, PharmD, Pharmacy Specialist, VA National Center for Patient Safety
In a 1997 article called "Discount Usability for the Web," Jakob Nielsen argued that, due to the rapid proliferation of technology, it was not practical to rely solely on highly trained usability engineers for the practice of user-centered design. Neilson advised the use of ‘discount usability’ methods whenever more ‘advanced and sophisticated’ methods were impractical during technology development. In fact, discount usability should be so pervasive in design processes that basic usability methods and principles should be included in public education...
Read More >
|
|
|
 |
Nursing And Usability Evaluation
Crystal Rojas RN-BC, MS, PHN, Informatics Nurse Specialist, Greater Los Angeles VAMC
A Revolution
Health information technology is revolutionizing the way we interact with health-related data. VA has a rich history in informatics with current efforts focused on modernizing its electronic health records and harnessing data both within VA and with partners. VA clinicians, especially nurses, will need to be a part of this revolution in order to ensure health IT (HIT) supports nurses in providing Veteran-centric care. Nurses comprise the largest group of healthcare providers employed in all healthcare delivery settings and are therefore the major group of electronic health...
Read More >
|
|
|
 |
Introducing VHA HFE Personas:
Who Are They and How Can You Use Them?
Ashley Cook, Human Factors Engineer, Jane Robbins, MBA, Human Factors Engineer, John W Brown, MS, Usability Specialist, & Nancy R. Wilck, Program Manager, HFE, OIA
Veterans, family caregivers and health care providers use and act on the information and features provided via VHA’s HIT products. If users cannot find what they need, understand what they find, and use applications effectively, efficiently, and safely, they will not be satisfied, will abandon use or will employ potentially unsafe workarounds. To improve care and outcomes, HIT products must work well for the people...
Read More >
|
|
|
 |
Call For Volunteers To Improve The Usability of VA Health IT Systems
Dale Ryan, MS, RN, Informatics Nurse Specialist, Health Solutions Management(HSM), OIA, Scott Wood, PhD, Health System Specialist, Informatics Patient Safety, OIA, & Jennifer Herout, PhD, Human Factors Engineer, HFE, OIA
VHA is moving forward with the development of a new health record, the electronic Health Management Platform (eHMP). In parallel, there are dozens of provider facing mobile apps in development, as VHA is rolling out mobile devices to sites across the country. Additionally, VHA is exploring how emerging health technologies, such as the IBM Watson cognitive system, could support VA clinicians in providing care. This article will discuss the need for end users to participate in these efforts, how user participation is critical to a user-centered design process, and how VA clinicians can...
Read More >
|
|
|
 |
Human Factors Educational Opportunities Spotlight
Ross Speir, Program Manager, HFE, OIA
This Spotlight supports the theme of encouraging VA clinicians to have a more active role supporting HIT systems usability. Perhaps the first step for interested clinicians is to become familiar with key concepts, processes, and methods of usability engineering. Fortunately, there are some excellent educational materials available in the Talent Management System for VA employees and registered...
Read More >
|
| |
| Back to top of article summary | Back to top of newsletter |
|
An Interview with David Eibling, MD
Christopher Petteys, MBA, Project Coordinator, Human Factors Engineering (HFE), Office of Informatics and Analytics (OIA)
Dr. David Eibling is an otolaryngologist at VA Pittsburgh Healthcare System (VAPHS). He is also a distinguished Professor at the University of Pittsburgh’s Department of Otolaryngology where he shares his wisdom and knowledge with Ear, Nose and Throat (ENT) residents, medical students, and others. Dr. Eibling has a passion for patient safety and the discipline of Human Factors Engineering.
- What is your role in the Veterans Health Administration (VHA)?
-
I have been a practicing otolaryngologist in VAPHS’ ENT department since 1990 when I was recruited to the University of Pittsburgh from an Air Force career. I was chief of the ENT department from my arrival until about 3 years ago when I stepped down to provide an opportunity for a younger otolaryngologist to develop leadership skills. At VAPHS, I have, and continue, to provide clinical care, including operative care, and teach ENT residents, medical students, and others. I am on the faculty of the University of Pittsburgh and am the vice-chairman for education of my department. In the past I did some clinical work at the university, but for the past 7 years have restricted my practice completely to VA.
In 2008, VAPHS was designated as a site for the VHA Inter-professional Fellowship in patient safety. I have directed the VA Pittsburgh Fellowship since that time, and am lucky to have recruited Jamie Estock, who is an outstanding co-director. This teaching endeavor now constitutes a large, and ever-growing, part of my academic efforts; and represents one of the most rewarding parts of my professional life.
- How were you introduced to the concept of Human Factors?
-
My engagement in Human Factors began as a transition through the IT world, from doing minimal computer coding in the early 1980s, to setting up surgical computer packages for a now-closed Air Force hospital in Germany in the mid-80s, and conducting a large cancer database conversion from Apple to IBM in the late 80s. However, I began to realize my work with computers was interfering with my practice, so after that I shifted my focus back to serving my patients.
With a very active outpatient practice, typically averaging 600 encounters per month and in addition to a busy ENT surgical practice, I relied heavily on paper-based records that consisted mostly of diagrams and sketches. During residency we had been taught to use standardized drawing tools, not only for clinic visits but also to illustrate our hand-written operative notes. This strategy enabled me to see as many as 80 to 100 patients per day, minimizing documentation time to a couple minutes per encounter. As I carried this strategy with me to Pittsburgh, I sometimes think about the thousands of archived paper files in storage.
In the mid-1990s, at the VA Butler Healthcare facility, a change began to occur when I first began to use the File Manager database within the Decentralized Hospital Computer Program (DHCP) - a DOS-like predecessor of the Veterans Health Information Systems and Technology Architecture (VistA). I was no longer able to utilize paper-based sketches, and this new paradigm dramatically reduced my productivity. The introduction of Computerized Patient Record System (CPRS) in 2000 resulted in some improvement, but the ability to create cognitively intuitive visual reports was permanently lost, and has never been replaced. I am now roughly 20% as efficient as I was in the paper-based sketch days. Not only does it take longer to generate reports, interpreting text reports, especially for a specialty that is highly visual, requires conversion of these reports to visual models. Although the ability to store images in VistA Imaging is helpful, images do not reproduce the cognitive value of a sketch. To say I was frustrated is an understatement.
I recognized that I needed to do something, so I took a two month mini-sabbatical in the Visual Information Center at the School of Information Sciences at the University of Pittsburgh. My collaboration with the people I met there represented my first introduction to human factors. Through these contacts I began to actively read some of the human factors literature, and almost immediately realized that what I was really interested in was how information transfer to critical people impacted patient safety. The rest of my transition to a human factors advocate was a natural progression of reading, communicating with interested colleagues, in and out of medicine, and attending National Human Factors Ergonomics Society meetings. Although I am still frustrated, I am now doing something about it, chiefly by mentoring and encouraging others to embark on human factors.
- How do you use/employ human factors in your work?
- As a practicing physician and teacher I use my daily clinical experiences as an opportunity to point out the ways in which human factors principles could be used to evaluate and improve safety for our patients. As an advocate, I use every opportunity to do just that. For example, consultation with human factors experts was the primary theme of a recent keynote address to a national ENT organization. This keynote address, “When More Than the Patient is Ill: Healing Sick Systems,” was delivered last May and the manuscript has been accepted and will be published this year in The Laryngoscope.
- What human factors – based project do you feel made the biggest impact in VHA? Why?
-
This question is difficult to answer because of my involvement in a wide range of projects over the past 25 years; however, the biggest impact was the introduction in 2001, of preoperative site marking and time-out at both VAPHS and Philadelphia VAMCs before adoption elsewhere. VAPHS’ former Chief of Anesthesia, Rick Bjerke and I had heard through the VISN 4 Surgical group of the site-marking process being recommended by the orthopedic group. We decided to implement our own system, even though we had not had any trigger events, but it seemed to be a good idea. We tried several different paradigms, including stickers, which initially failed since they came off during site scrubs, but eventually took hold. We could never have predicted the impact.
- Where do you see the greatest potential for the application of human factors principles in VHA?
-
VHA, as the largest integrated healthcare system in the United States, has the greatest opportunity and responsibility to infuse human factors expertise into all aspects of health care delivery. The theme of designing systems and artifacts for human users to improve their performance are well known to the readers of this piece, but to date have not taken hold in the industry as a whole. I am optimistic, however, that as healthcare workers begin to see changes come about as a result of human factors input, they will begin to expect the devices and products they use in their daily work be designed for human users like themselves. For example, both the Patient Safety Center of Inquiry and Center for Medical Product End-User Testing directed by Jamie Estock at VAPHS, evaluate the risk of use error in new products. The recently accepted (but yet unpublished) study of intravenous medication labeling in a simulated operating room is precisely the sort of study which VA can – and should - do to improve product design to reduce human use error.
Other opportunities include leveraging VA purchasing power to drive product change, such as in medication labeling. There are currently approximately 27 different color combinations for the common medication omeprazole, possibly leading to an increased potential for medication error. Based on its size, VHA could easily stipulate designs, labeling, and medication marking in all its contracts, and potentially ultimately impact safety nation-wide.
- Have you seen changes in the interest in or awareness of human factors in VA? What are they?
- Unfortunately, I see relatively little awareness of human factors principles outside of the National Center for Patient Safety (NCPS). The educational opportunities – and challenges – are enormous. It is unlikely that medicine – or for that matter, VHA, will ever achieve the same awareness of human factors as is to be found in other safety-critical fields such as aviation or energy, in my lifetime. However, widespread awareness of successful examples such as those I mentioned earlier, with dissemination of this new knowledge, has the potential to increase the appreciation of the role human factors plays in process and device design. I believe with education and leadership regarding the value of human factors, we will see improvements in knowledge and resource allocation. Perhaps more critical is our opportunity to impact medical and nursing students as well as other healthcare workers in training. I also believe VHA is the only institution in US healthcare where this is possible.
|
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Local Application and Transmission of User-Centered Design Principles
Tim Arnold, PharmD, Pharmacy Specialist, VA National Center for Patient Safety
In a 1997 article called "Discount Usability for the Web," Jakob Nielsen argued that, due to the rapid proliferation of technology, it was not practical to rely solely on highly trained usability engineers for the practice of user-centered design. Neilson advised the use of ‘discount usability’ methods whenever more ‘advanced and sophisticated’ methods were impractical during technology development. In fact, discount usability should be so pervasive in design processes that basic usability methods and principles should be included in public education curriculum. Eighteen years later, usability principles are seldom included as part of a standard education; and neither are they included in most graduate or medical school curriculums.
For the development of VA health information technology, the Human Factors Engineering (HFE) program, the NCPS, and several other groups within VA recognize the value of human factors and user-centered design. These groups have taken substantial steps to increase the organization’s awareness of usability principles. The following narrative describes a VA clinician's journey through the local application and transmission of concepts specific to user-centered design.
How a pharmacist applied user-centered design principles at the local level
My first exposure to human factors engineering came during a NCPS inter-professional patient safety fellowship boot camp. As Dr. John Gosbee discussed in the Winter 2013 HFE Newsletter, this exposure marked the beginning of a brain flip for me. I began to see the design of technology from the perspective of how well it supports (or does not) the human components of a work system. During my time as a VA NCPS patient safety fellow and afterwards, I began utilizing user-centric design techniques at local VAMCs to evaluate cognitive memory aids, clinical decisions support tools, and delivery devices. I collaborated with end users (including novices) to generate a conceptual model of an application; improved user interface designs based on usability heuristics, and performed cognitive walkthroughs with clinicians to analyze design effectiveness. I also conducted usability evaluations of CPRS menus/templates designed to support clinical decision making and medication selection. These evaluations were successfully carried out by following the approach outlined by Alissa Russ and colleagues in "A Rapid Usability Evaluation (RUE) Method for Health Information Technology," (2010) which provides a framework for a low cost and efficient means for conducting an usability evaluation on locally developed HIT tools. My experiences learning and applying usability methods have led me to conclude that clinicians can and should have an integral role in designing safer and more user-centered systems.
Why it's important to develop user-centered design expertise at the local pharmacy level
The impetus for exposing pharmacists to human factors concepts lies in the fact that automated and technological systems are increasingly entwined in pharmacy work processes, including those related to electronic health records, ordering, and medication verification systems (VistA/CPRS), infusion pump drug libraries, barcode medication administration systems, and automated dispensing cabinets, to name a few. Components of VistA/CPRS such as the local drug file, orderable items, and order dialogs are examples of items in which modifications are common; this adds to variability at the local level. In addition, the interconnectedness of these systems with VA and consumer-off-the-shelf products (COTS) creates another level of complexity and a challenge to understanding how these systems support the users' tasks. Pharmacy personnel setup components and modify settings in these systems which have the potential to impact how and what information is presented to the user at the interface. In addition, pharmacists in clinical application coordinator (CAC) or pharmacy informaticist positions have roles specific to these tasks. Therefore it seems prudent to expose the pharmacy workforce to principles of user-centered design.
Transmission of user-centered design principles to up-and-coming leaders in pharmacy
What better place to expose and develop expertise in user-centered design than in a medication safety rotation during a pharmacy residency? We inserted these concepts didactically and experientially as an elective addition to an existing medication safety curriculum for pharmacy residents. This portion of the curriculum contained articles on principles in human factors, a review of Nielsen's 10 usability heuristics and a facility tour in search of potential design concerns. Residents were required to perform a preliminary heuristic evaluation, walkthrough, and subsequent discussions of locally grown products. As part of the overarching residency curriculum, pharmacy residents are often required to present journal article reviews. This is typically a systematic review of an article steeped in pharmacotherapeutics. Sample articles related to user-centered design principles and applicable to pharmacy were provided as potential articles for presentation at a pharmacy journal club. Not only is this a change from the traditional pharmacy journal club, but it seemed to be an initial point of exposure for participants. In addition, recent exposure to human factors concepts may have driven the transformation of the journal club experience into an interactive hands-on activity. Pharmacy residents often find subsequent work within VA; therefore, immersion in principles of user-centered design during residency is another step in building local expertise in human factors.
A few things learned along the way
- Local modifications, variability, and product development necessitates local user-centered design expertise.
- One doesn't necessarily have to be a human factors engineer or clinical informaticist to lead a design effort, but early and ongoing discussions with subject matter experts can be helpful for understanding design processes and for understanding functional confines.
- Finding a mentor(s) with expertise in human factors within VA can be helpful and a lot of fun.
- Strategic, cautious planning and gradual application of user-centered design principles within an organization impacts willingness to embrace. I have witnessed this shift in acceptance in an organization.
- Building an informal team of interested individuals can help with this momentum. It's okay to be choosy. "In it for the long-haul" attitudes and super civil behaviors work well.
- As local expertise grows, the pool of evaluators grows, along with a subsequent increase in the recognition of usability issues.
- It's acceptable to evaluate one's own design but recognize that there will be unintentional bias. It’s helpful to better understand the pros and cons of both evaluating one's own design and undergoing third-party evaluation.
- "We become what we behold. We shape our tools and thereafter our tools shape us"
- Marshall McLuhan.
|
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Nursing And Usability Evaluation
Crystal Rojas RN-BC, MS, PHN, Informatics Nurse Specialist, Greater Los Angeles VAMC
A Revolution
Health information technology is revolutionizing the way we interact with health-related data. VA has a rich history in informatics with current efforts focused on modernizing its electronic health records and harnessing data both within VA and with partners. VA clinicians, especially nurses, will need to be a part of this revolution in order to ensure health IT (HIT) supports nurses in providing Veteran-centric care. Nurses comprise the largest group of healthcare providers employed in all healthcare delivery settings and are therefore the major group of electronic health record (EHR) users. Nursing plays a vital role not only because of their numbers but also their intimate understanding of clinical workflow.
The Nurse Role
The Institute of Medicine (IOM) emphasizes the importance of nursing’s role in healthcare transformation, asserting that nurses should be in a full partnership with other healthcare professionals to redesign American healthcare. As full partners, nurses must help drive the changes that affect them most. As primary consumers, they are significantly affected by EHR software design and usability.
Nurses already struggle with limited time to perform the substantial duties of their work. Electronic health records are central to health IT and need to be both usable for nurses and relevant to their practice. While nurses and other clinicians have traditionally been passive users of EHR technology, VA nurses should be active in decision-making about VA HIT systems. It is imperative that they provide valuable user input for EHR requirements, design, purchase, evaluation and implementation to ensure that technology is usable and supports clinical workflow.
The Role of the Informatics Nurse Specialist (INS)
The informatics nurse specialist (INS) can play a central role in HIT system usability. These individuals are trained to bring together fields of nursing science, computer science, and information science to improve the nursing practice. This unique perspective of the INS can streamline the processes and reduce the costs of applying usability to the development, procurement, and implementation of HIT systems. The INS can leverage clinical expertise, informatics knowledge, and IT experience to facilitate communication between system developers, usability engineers, and end users.
To ensure a HIT system will meet the needs of intended users, an evaluation of system usability should be carried out. Usability evaluations can take place during system design, purchase, deployment, and organization-specific configuration. The National Institute of Standards and Technology (NIST) released an applicable document that outlines formal procedures for evaluating the usability of EHRs, titled the EHR Usability Protocol (EUP). The following three-staged framework, based on the EUP, describes the role of the INS as a central figure supporting EHR usability. This framework represents the usability evaluation of an EHR software development project at a stage before full implementation.
- Stage 1: EHR Application Analysis
- STEP 1: CREATE APPLICABLE USE CASE SCENARIOS OR TEST SCRIPTS
As a bridge between technical and clinical domains, the INS has access to draw upon practicing clinicians to formulate applicable use case scenarios. The INS has a unique skill set necessary to vet these scripts for appropriateness and accuracy. The scenarios should represent the spectrum of clinical tasks that are high frequency, common to practice, critical to work, and complex in nature.
- STEP 2: CREATE APPLICATION USER PROFILES
With a central role in the VA health system, the INS can identify the range of user types (both primary and secondary users) that the HIT system must support. Our systems are highly interwoven and it is important to identify users both upstream and downstream in the clinical workflow. The Human Factors Engineering Office recently launched a series of User Personas based on actual user data and anecdotes. These have great potential for VA clinical software development, and the INS should be involved in refining the personas to ensure all key roles in the user populations are represented.
- STEP 3: IDENTIFY A REALISTIC USE ENVIRONMENT
Effective design and testing requires development teams to understand the contexts and environments where the HIT system will be used. For instance, effective usability testing will account for noisy, chaotic nursing stations that are common at medical centers. System designs must account for real differences across our VA Medical Centers. The INS can contribute to software designed to meet a broad range of needs.
- STEP 4: DETERMINE CRITICAL SAFETY-RELATED ISSUES
This concept is reinforced throughout the project life cycle of software development, and the INS can work to identify near misses when doing usability validation. The INS can also test the ability of the system to reduce likelihood of human error.
- STEP 5: PRELIMINARY ASSESSMENT OVERVIEW
In this step, the INS prepares a document that includes information from steps 1-4. This toolkit can be used by testers to independently evaluate the EHR software with relevant scenarios, a realistic environment, and critical safety related issues in mind.
- Stage 2: Expert Review
- Expert review can be performed by both usability experts and the INS with usability expertise. These reviews include exercises like heuristic evaluations, and cognitive walkthroughs. It is suggested that nurses learn fundamental usability evaluation skills and combine these with clinical wisdom to contribute meaningful software development feedback. General software exploration often yields meaningful feedback as well to assess how our software modules and workflows work together as we need devices and interfaces that support workflows in all VA clinical areas.
- Stage 3: Interface Validation Testing
- The INS can support usability engineers with the design and setup of rigorous usability validation testing by ensuring clinical relevance and accuracy of these tests. The INS also plays a key role in determining the severity of usability issues uncovered during testing and identifying design solutions that reduce the risk of delaying application release.
For more details of this proposed framework, please view the article published in the journal CIN: Computers, Informatics, Nursing
Looking Forward
This is an exciting time for VA nurses in the arena of Informatics and EHR development. The INS acts as a bridge between nurse end users and software developers, but this is a call to action for more VA nurses to take a seat at the development table through project participation and informatics training. Usability is a collective duty among end users, the INS, and software developers. Nurses want EHRs that help them to work smarter, do not bury needed content, and are easy to read and understand. As HIT is fundamentally changing the way nurses practice, it is likely that more nurses will seek leadership positions in the field of informatics. There are also many opportunities within VA to develop professional skills in the field. Some of these include VA sponsored AMIA 10x10 course, Introduction to Health Informatics course (101) and the Health Informatics Lecture Series (301), all developed by the forward-thinking Workforce Development team under Health Solutions Management.
|
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Introducing VHA HFE Personas:
Who Are They and How Can You Use Them?
Ashley Cook, Human Factors Engineer, Jane Robbins, MBA, Human Factors Engineer, John W Brown, MS, Usability Specialist, & Nancy R. Wilck, Program Manager, HFE, OIA
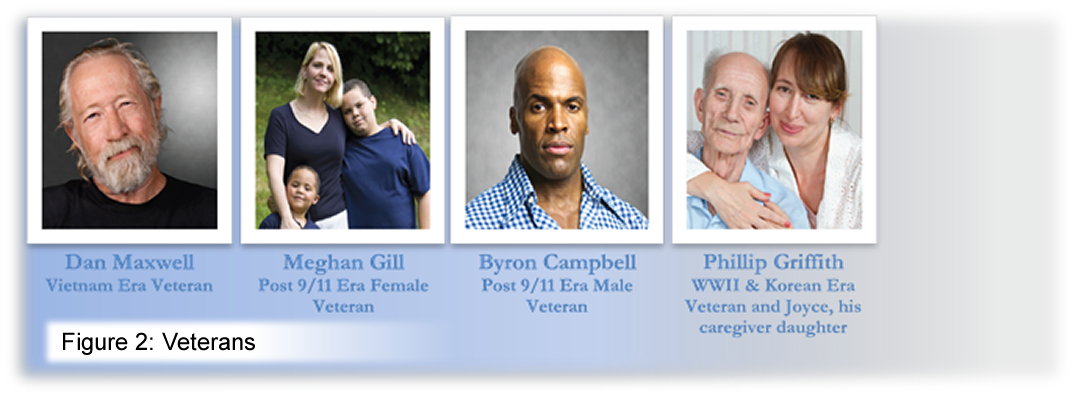
Veterans, family caregivers and health care providers use and act on the information and features provided via VHA’s HIT products. If users cannot find what they need, understand what they find, and use applications effectively, efficiently, and safely, they will not be satisfied, will abandon use or will employ potentially unsafe workarounds. To improve care and outcomes, HIT products must work well for the people, illustrated in Figure 1, who use them.
 Ideally, to produce the most positive user experience possible, actual end users participate throughout the entire software development lifecycle in order to influence product design. This full integration of end users in every design decision is not practical in most cases. As a result of limited involvement of end users, many decisions are made by stakeholders and development teams without their input. Ideally, to produce the most positive user experience possible, actual end users participate throughout the entire software development lifecycle in order to influence product design. This full integration of end users in every design decision is not practical in most cases. As a result of limited involvement of end users, many decisions are made by stakeholders and development teams without their input.
In the absence of end user engagement, development teams often interject on their behalf with assumptions or partial knowledge of people who might use the product. Designers, developers, and other stakeholders often use phrases starting with "The user might…" in order to define functionality for a product. A key problem is that members of teams often lack an accurate and/or shared understanding of their intended end users. For example, some team members may think in terms of the power user, while others think in terms of a nursing student who has worked at VHA for mere weeks. The end result of this “elastic user” can become a jumble of features that doesn’t suit anyone’s needs.
To address this knowledge gap, VHA HFE has developed an initial suite of data-backed personas as a tool for more accurate decision making on behalf of users. These personas act as an “empathetic bridge” between software development teams and end users, enabling decisions that produce the best user experience possible.
The HFE Personas team is pleased to announce the “birth” of our first seven personas. The Veterans are represented by four personas, shown in Figure 2 and the Clinicians are represented by three personas, shown in Figure 3:
 |
|---|
HFE’s personas are fictional characters that were distilled from user research and are intended to aid in the development of usable and useful HIT at VA. They represent the needs of larger groups of people who use VHA HIT systems and mobile apps, communicating their needs and expectations. In producing these personas, HFE conducted extensive user research and analysis on VHA clinicians, Veterans and family caregivers who use VHA services. They were drafted based on analysis of data collected from external and internal sources and then validated with Veterans and Clinicians.
 |
|---|
The personas should be seen as living, breathing, characters because they work best when they permeate all team discussions about the users’ interaction with the product. Development team members should refer to them by name whenever they discuss “the users.” The team effectively invites the personas to become “members” of development teams, acting as readily accessible and interactive forms of user research as teams strive to keep the user at the center of their product development.
There are a many opportunities to incorporate personas into team activities  without significant modifications to existing software development processes and/or methodologies. Figure 4 shows a sample set of various user personas. In addition, the list below provides ideas for getting started with personas: without significant modifications to existing software development processes and/or methodologies. Figure 4 shows a sample set of various user personas. In addition, the list below provides ideas for getting started with personas:
-
Help identify HIT solutions to address program challenges. Program offices can employ personas along with Story Mapping or other visioning techniques to help identify potential HIT solutions to address program challenges.
-
“Interview” personas about their needs. When developing or planning to elicit requirements for inclusion in the project’s Business Requirements Document (BRD), “interview” personas about their needs to produce a more accurate draft for validation by actual end users.
-
When prioritizing features, “ask” the personas for their thoughts. For example, prepare matrix mapping persona priorities to features in order to inform the project team as decisions are made for sequencing development.
-
Prepare scenarios (or use cases) demonstrating how the personas will utilize the feature(s). This aids in creating system flows and wireframes that meet user information and functionality needs.
-
Use personas as the subject of user stories. In lieu of the generic “As a user…” statement at the opening of user stories, use the personas as the subject of the user stories. This can immediately provide reference to user needs, perceptions, constraints, etc. which can be critical when estimating and/or implementing a particular story.
-
“Ask” the personas for their input when resolving design disputes. Refer to personas to help overcome disputes within the team or between stakeholders over specific design decisions. Avoid debates that begin with the amorphous “user” (e.g., “The user isn’t going to understand this label.”). Instead, talk about the persona’s needs (e.g., “Dan will understand this label because [insert applicable reference from Dan’s persona profile].”). Having teams refer to the needs, motivations, behaviors and constraints of personas can help ensure that the system is designed to satisfy those users’ requirements.
-
Test from the personas’ perspective. Consider building test beds of data for each persona. This enables efficient and effective Test Driven Development (TDD) against user centered acceptance tests. It also allows testers and project stakeholders to test from the perspective of the personas, ensuring that their feedback is valuable in the actual context of use.
HFE personas are available in low resolution and high resolution formats on the HFE Body of Knowledge User Persona Library. On the same page, you can find a detailed “How to Use Personas” document and an “HFE Brown Bag Presentation” if you’re interested in additional reading. Please note that our SharePoint site requires a va.gov email account for access. We are very interested in your thoughts on the personas and have included a feedback link in the personas package.
Persona use and development are services of the Human Factors Engineering Office. If your team needs assistance in using the personas or if the personas provided don’t fit the needs of your VHA health IT product, HFE can work with you to create one that does. For more information on engaging with VHA HFE to prepare additional personas, support your software design or conduct usability inspections, please contact:
Nancy Wilck VHA OIA | Human Factors Engineering
Email: nancy.wilck@va.gov
Office: (202) 330-1818
For more information on personas or how to use them, please join us at the HFE’s Office Hours or contact the persona team:
John Brown VHA OIA | Human Factors Engineering
Email: john.brown14@va.gov
Office: (615) 320-6293
|
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Call For Volunteers To Improve The Usability of VA Health IT Systems
Dale Ryan, MS, RN, Informatics Nurse Specialist, Health Solutions Management (HSM), OIA, Scott Wood, PhD, Health System Specialist, Informatics Patient Safety, OIA, & Jennifer Herout, PhD, Human Factors Engineer, HFE, OIA
VHA is moving forward with the development of a new health record, the electronic Health Management Platform (eHMP). In parallel, there are dozens of provider facing mobile apps in development, as VHA is rolling out mobile devices to sites across the country. Additionally, VHA is exploring how emerging health technologies, such as the IBM Watson cognitive system, could support VA clinicians in providing care. This article will discuss the need for end users to participate in these efforts, how user participation is critical to a user-centered design process, and how VA clinicians can participate in VA health IT system design and testing.
Early and continual focus on end users has long been a core principle for building usable systems (Gould & Lewis, 1985). The systematic involvement of end users in the software design process (such as that outlined in ISO 9241: Human-Centered Design for Interactive Systems) contributes to useful, usable and safe products by identifying early in the process which system designs work and which don’t. To this end, VHA has created a mechanism by which VA clinicians can volunteer their time to support various HIT development efforts.
VistA Evolution
The VistA Evolution team is conducting biweekly Quick Review sessions to hear end user feedback on new design features. These sessions present a feature or wireframe for early feedback, before coding is complete. This type of feedback is collected virtually and sessions last less than an hour. Feedback will provide the developers with a perspective of how features may be of benefit to clinician workflow.
In addition to these Quick Review studies, the team will be evaluating newly developed software before it is released to IOC, partner, and early adopter sites. These tests will last 1-2 hours and will also be done virtually. They will allow the development team to better understand relationships between the individual features.
Mobile Applications
The fast introduction and growth of mobile apps being developed for providers with tablets and smart phones is making way for various opportunities in the development process. VA clinicians can now provide feedback on mobile apps, including help with scoping the app to match workflow, commenting on early designs, and testing close-to-final products.
Feedback results gathered during usability sessions will be used to improve the usability of continuing software development. Any input provided is greatly valuable. Sessions are currently slated to take place at least every two weeks with most being held virtually. Participation is completely voluntary, the individual feedback is kept confidential, and names will not be associated with any comments or results.
Clinical Reasoning System Assessment (CRSA)
A Clinical Reasoning System is an emerging class of technology that can quickly extract key information from the large data sources (such as an EHR and the entire medical literature) and then present that knowledge in a manner and form that supports how clinicians naturally reason and make inferences in a clinical setting.
The CRSA project is a two year pilot that utilizes the IBM Watson technology to assess the value of clinical reasoning systems to VA clinicians. The project is looking for volunteers to support various aspects of this assessment. For instance, determining if this technology can understand complex clinical questions in natural language and then formulate a meaningful response from the medical literature is one area of need. Volunteers will be asked to shape how the technology will respond to inquiries about the patient, searching the full electronic medical record of a patient and displaying the results, at the point of care. This project is looking for VA clinicians to serve in both ad hoc and long-term roles.
What volunteers should expect
VA clinicians willing to contribute their time and expertise to HIT design and usability testing can submit their names to a Usability Participant list. When a software development project requires input from end users, someone from HFE will pull the appropriate user types from the database and send an invitation to participate. Invitations will typically include
- A brief description of the HIT project (the type of app or functionality being developed)
- A description of the type of user feedback needed (user needs assessment, participatory design session, usability testing, etc.)
- The available dates and times from which participants can select (sessions are typically only an hour long)
Participants are expected to provide honest, open feedback. Frequently, participants are asked to provide detailed, contextual feedback about the HIT system. For instance, the project team may ask how a proposed design would affect the clinical workflow; or they may ask for scenarios that would be problematic for the design. If you would like to be contacted for volunteer participation please visit the Usability Participant List Sign-up and fill out the brief questionnaire to provide contact information. Doing so will enable you to be contacted for future usability testing and other potential collaborative opportunities.
Sign up to become a Usability Study Participant!
|
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
 Human Factors Educational Opportunities Spotlight Human Factors Educational Opportunities Spotlight
Ross Speir, Program Manager, HFE, OIA
This Spotlight supports the theme of encouraging VA clinicians to have a more active role supporting HIT systems usability. Perhaps the first step for interested clinicians is to become familiar with key concepts, processes, and methods of usability engineering. Fortunately, there are some excellent educational materials available in the Talent Management System for VA employees and registered contractors.
In 2012, VA partnered with American Medical Informatics Association (AMIA) to develop an online Health Informatics Certificate Program. The purpose of this ‘AMIA 10x10’ course is to familiarize VA employees with a broad range of health informatics topics that would promote the acceleration, implementation, and support of HIT innovations to improve health care delivery. One of the topics in this course is Human Factors Engineering, and materials for this topic include 3 one hour-long lectures delivered by experts in the field of human factors applied to the HIT domain. I highly recommend these lectures for VA clinicians wanting to become actively involved in the usability of VA HIT.
Models, Theories and Practices of Human Computer Interaction (TMS # 11265) outlines principles and approaches used to understand the human aspects of the Human Computer Interaction (HCI), including the cognitive, social, and environmental factors that impact the effective and safe interaction with technology.
Interface Design Standards and Principles (TMS # 11265) provides guidance for developing and evaluating user interfaces. This lecture describes some design issues related to HIT and provides heuristics for improving design usability.
Human Computer Interaction: Evaluation, Usability Testing, Study Design and Methods (TMS # 11265) provides an overview of the usability methodology, describes how to develop and run a usability study, and discusses what can be learned from the results of a usability study.
Becoming familiar with these topics will enable you to become a strong advocate for VA HIT usability. Enjoy!
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
 |
|

