 |
 |
In this issue of the newsletter, we present an array of articles that highlight different aspects of Human Factors Engineering (HFE), including HFE facts vs. fiction, patient safety, workarounds, education, an interview with human factors expert Dr. John Gosbee, as well as a new feature: Mobile App Design Brief. We'd welcome your feedback on the content of our current newsletter, as well as your suggestions for future content. Email us to provide feedback on the newsletter.
- Jason J. Saleem, PhD, Editor-in-Chief.
|
 |
 |
Risks to Patients Due to Incorrect Patient Record Selection
Jean Krieg, BS, Management Analyst, Lesley Taylor, BS, Management Analyst, Scott D. Wood, PhD, Health System Specialist, Jeanie Scott, BS, Director Informatics Patient Safety (IPS), Office of Informatics and Analytics
Patient misidentification can occur at almost any point in the health care process, with or without the use of Health Information Technology (HIT). The selection of patient records is a common task while using Electronic Health Record (EHR) systems in which patient misidentification is an ever-present risk. When errors do occur in patient record selection, several unintended consequences can result, including information documented...
Read More >
|
- Upcoming Events
-
2014 Symposium on Human Factors and Ergonomics in Health Care: Leading the Way, March 16-19, 2014, Chicago, Illinois.
-
2014 Joint Summits on Translational Science, San Francisco, April 7, 2014 - April 11, 2014
- Informational Links
- Human Factors Engineering (HFE) within the Veterans Health Administration (VHA) Office of Informatics and Analytics, Health Informatics Division seeks to increase awareness of human factors products and services among clinical end-users and other stakeholder groups. This quarterly newsletter serves to engage these communities in shared communication and collaboration around human factors-related issues.
Access and review previous issues of this newsletter
- Editor-in-Chief:
- Jason J. Saleem, PhD, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Managing Editor:
- Christopher Petteys, MBA, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Editorial Board Members:
- Michael W. Smith, PhD, Houston VA HSR&D Center for Innovations
- Rachel Wiebe, RD, CPHQ, iEHR Staff Office, Health Informatics, Office of Informatics and Analytics
- Linda C Williams, RN, MSI, VA National Center for Patient Safety
- Scott D. Wood, PhD, Informatics Patient Safety, Office of Informatics and Analytics
|
 |
 |
What You Need To Know: 5 Key Facts About Human Factors In Health Care Improvement
Highlights from the article: "The Science of Human Factors: Separating Fact from Fiction."
Rachel Wiebe, RD, CPHQ, Patient and Clinician Experience Analyst, iEHR Staff Office, Health Informatics, Office of Informatics and Analytics
Congratulations to our VA colleague Dr. Alissa Russ, research scientist and human factors engineer at the VA Health Services Research & Development (HSR&D) Center for Health Information and Communication, at the Richard L. Roudebush VA Medical Center in Indianapolis, Indiana who, with her...
Read More >
|
|
|
 |
"Flipping" Health Care Professionals' Way of Thinking about Patient Safety:
An interview with Dr. John Gosbee
Christopher Petteys, MBA, Program Coordinator, Human Factors and Linda C Williams, Program Specialist, RN, MSI, VA National Center for Patient Safety
From 1999 to 2006, Dr. Gosbee worked at VA's National Center for Patient Safety (NCPS). During his time with NCPS, he led the development of patient safety and Human Factors Engineering residency and medical school curriculum. He also led the Human Factors Engineering analysis of adverse events and close calls involving medical devices and software, including as the liaison to companies to rectify...
Read More >
|
|
|
 |
Workarounds Illuminate Gaps in the EHR
Jason J. Saleem, PhD, Technical Information Specialist, Human Factors Engineering, Office of Informatics and Analytics
Workarounds are nonstandard procedures that people develop because of real or perceived limitations in system or workflow design. Over the last several years, my colleagues and I have investigated HIT workarounds...
Read More >
|
|
|
 |
Health Care Human Factors Curriculum: Improving Patient Safety by Making Human Factors Engineering Accessible
Kristen Miller, DrPH, MSPH, Research Fellow, VA National Center for Patient Safety (NCPS) Tandi Bagian, MSE, Director, Human Factors Engineering Division, VA NCPS
Preventable or avoidable adverse events can often be attributed to a failure to follow recognized, evidence-based best practices or guidelines at the individual or system level. Studies of adverse patient incidents have heightened our awareness of the...
Read More >
|
|
|
 |
Mobile App Design Brief:
Navigation Bar Design Considerations
Donna Harrigan, BA, Management and Program Analyst, Human Factors Engineering, Office of Informatics and Analytics
The new Mobile App Design "brief" series will highlight best practices in action in VA for mobile User Interface (UI) design certifications. This first brief focuses on navigation bar design.
Who likes intuitive, easy to use apps? I'll venture out on a limb and say...
Read More >
|
| |
Back to top of article summary | Back to top of newsletter
|
|
Risks to Patients Due to Incorrect Patient Record Selection
Jean Krieg, BS, Management Analyst, Lesley Taylor, BS, Management Analyst, Scott D. Wood, PhD, Health System Specialist, Jeanie Scott, BS, Director Informatics Patient Safety (IPS), Office of Informatics and Analytics
Patient misidentification can occur at almost any point in the health care process, with or without the use of Health Information Technology (HIT). The selection of patient records is a common task while using Electronic Health Record (EHR) systems in which patient misidentification is an ever-present risk. When errors do occur in patient record selection, several unintended consequences can result, including information documented in the wrong patient record and information not being documented in the intended patient record. Both associated patients are then at risk for misdiagnosis, incorrect or unnecessary care, or delay of care. Most cases can be traced back to underlying human factors issues, either in the health care workflow and the HIT design. In this article, we explore how simple design choices can have a large impact on patient safety and suggest an approach to minimizing risk to patients.
Incorrect patient record selection is a relatively frequent form of an adverse event. A controlled study in order entry interface design by Hettinger and Fairbanks (2012) found that 76 percent of providers did not recognize the occurrence of a patient selection error. In another study, Koppel (2009) found that "almost all residents reported having accidently entered orders in the wrong patient's electronic chart at one time. While these house officers uniformly reported catching their errors before closing the electronic chart, it goes without saying that they probably didn't catch the errors they did not notice." These studies demonstrate that incorrect patient record selection is a prevalent problem, not just in VA, but also in the broader health care community.
To help describe incorrect patient record selection issues from the human factors perspective, we characterize the steps as belonging to one of three action types: cognitive (remembering or deciding), perceptual (seeing, touching, hearing, etc.), or motor (keystrokes, mouse movements, finger taps, etc.), incorrect patient selection can result from errors stemming from any of these action types. However, to design effective interventions that target incorrect record selection, we have to understand which types of user actions are causing problems.
There are many ways to search for patients within an EHR, each of which presents a unique set of actions and risks. Figure 1 illustrates a common patient selection scenario based on searching for a patient's name. In this case, the user intends to enter an order into the record of Patient B. It begins with a cognitive action in Step 1, where the user decides which patient name to search (ZZTEST, PATIENT B). In Step 2, the user performs a motor action, typing the first few letters of the patients name into the search field. In response to this, the system populates the patient selection list, filtering out any names that do not contain the entered letters. Note also, in our scenario, that the system has a feature where the previously selected patient name (ZZTEST, LASTPATIENT) is displayed at the top of the list, irrespective of what is typed in the search field. In Step 3, the user then performs a perceptual task to find the desired patient in the displayed search list. In Step 4, the user then moves the cursor to the desired patient name and selects the record (actually two motor actions: move cursor and select name). The system then retrieves the selected record, switches to the patient record screen and displays the patient's record. At this point, Step 5, the user is expected to inspect the patient name and other demographic identifiers (a perceptual action) to verify that the record corresponds to the desired patient (a cognitive action).
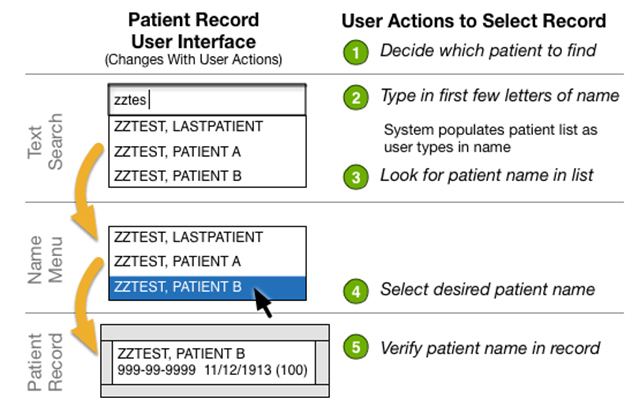
Figure 1. Typical user steps necessary to select patient record. The sequence of images on the left shows how the UI changes during a typical patient record search. The search begins with the user intention to select the record for a particular patient and ends when the patient record is displayed. The steps on the right represent the cognitive, perceptual, and physical actions a user performs to complete the task.
Errors can occur in any of the record selection steps. For example, action slips can occur by mistyping the patient name (Step 2), or by selecting the wrong name above or below the intended name (Step 4). Perceptual slips can occur by misreading Patient A as the intended record (Step 3), or not noticing discrepancies between the intended patient's identifiers and those in the record displayed (Step 5). If the user does not remember the intended patient name (Step 1), then this is considered a mistake because the entire plan is incorrect (as are all the steps that follow). The interface in Figure 1 creates a circumstance to easily select the last patient. Another classic type of mistake is when users incorrectly assume that their intended patient is the last patient selected from a workstation, causing them to select the wrong patient.
We recommend using an error-tolerant design framework to address incorrect record-selection and other forms of use error. The idea is to build a layered defense to eliminate or reduce hazards, minimize risk to patients, and support a sustainably-safe operational environment that is tolerant of human error and system failure:
-
Prevention – prevent use error when possible, for example, by not allowing incorrect or inappropriate actions (forcing functions).
-
Reduction - reduce use error when prevention is not entirely possible, for example, by designing larger button targets to reduce incorrect selection or requiring confirmation for safety-critical actions.
-
Detection & Identification - when use error does occur, ensure that the user can detect when something is not right and identify what specifically went wrong.
-
Correction - provide support for users to correct use errors and return to their primary tasks.
-
Mitigation - provide a means for users to mitigate the effects of use error if correction is not possible, such as requesting help from informatics support personnel.
-
Monitoring - monitor system usage after deployment to automatically detect hazardous or erroneous conditions and provide a means for users to voluntarily report adverse events.
Applying this framework to incorrect patient selection suggests several design changes to help minimize patient risk (we'll consider three aspects of the framework). First, although error prevention is usually difficult, if we remove the last-patient functionality from our example, it will remove the possibility for one important class of mistake, selecting the wrong last patient. This intervention also illustrates an important difference between patient safety and traditional human factors approaches: sometimes patient safety guidelines conflict with more familiar usability goals, such as efficiency of use. In this case, designers must make a tradeoff between perceived speed of use and minimizing risk of incorrect selection.
A second line of defense is to reduce errors that we cannot completely eliminate. For example, making patient information more salient may help reduce perceptual slips. Adding contextual information about patients, such as birthdate and age, can also provide cues to the user to help select the correct patient. To improve the verification step, patient identifiers can be made more visually salient on the patient record page itself, which would also help with detection of any of the errors discussed. An alternative design change would be to add an explicit confirmation step after Step 4, which could show additional identifiers and other contextual information, such as a photograph and/or attending physician. In one hospital, adding an explicit confirmation step and a mandatory 3-second delay reduced incorrect patient record selection by 70 percent. Again, this type of design choice represents a tradeoff between safety and efficiency.
A third line of defense is monitoring system usage to detect possible use error and to better understand which interventions are effective in reducing risk. For example, Adelman and colleagues (2012) demonstrated that monitoring orders that were discontinued and reordered on another patient within two hours of being signed was a good indicator of patient misidentification. Likewise, monitoring when users cancel confirmation dialogs would indicate that the dialog helped them detect a selection error. This type of data collection to detect erroneous usage patterns not only informs future designs, but can also be used to facilitate error correction by HIT support personnel.
Incorrect patient record selection is a prevalent form of use error that still challenges EHR designers. Analyzing adverse events from a human factors engineering perspective can go a long way towards developing effective design interventions that reduce risk to patients and improves usability for clinicians. Utilizing a comprehensive framework for error-tolerant design helps to identify gaps in defense against patient harm and helps us design more robust and effective health care systems.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
What You Need To Know: 5 Key Facts About Human Factors In Health Care Improvement
Highlights from the article: "The Science of Human Factors: Separating Fact from Fiction."
Rachel Wiebe, RD, CPHQ, Patient and Clinician Experience Analyst, iEHR Staff Office, Health Informatics, Office of Informatics and Analytics
Congratulations to our VA colleague Dr. Alissa Russ, research scientist and human factors engineer at the VA Health Services Research & Development (HSR&D) Center for Health Information and Communication at the Richard L. Roudebush VA Medical Center in Indianapolis, Indiana who, with her co-authors, recently published a thought provoking article in the British Medical Journal Quality & Safety, an international journal of health care improvements. The article is titled, "The science of human factors: separating fact from fiction."
Lead author, Dr. Russ, started her career as a biomedical engineer and changed career paths after a clinical internship in graduate school where she gained insight into the complexity of health care and became aware of the many patient safety concerns and risks in health care systems. Dr. Russ said she began asking herself, "Why am I doing bench research when there is so much fundamental work to be done to improve health care delivery systems?" She went on to complete a two year VA HSR&D post-doctoral fellowship in Indianapolis, where she specialized in Human Factors Engineering research.
Have you ever tried to answer the questions: What is human factors? What does it mean? What is it all about? Why human factors? How does it fit with health care? If these questions sound familiar to you or you have ever wondered about these topics, this journal article is for you!
Dr. Russ developed the idea for the journal article following a panel discussion on the topic of human factors education for health care professionals at the 2011 Human Factors and Ergonomics Society Annual Meeting. As the panel members began to plan and discuss their presentation, they soon recognized they had many shared experiences about human factors misconceptions, and as a group, they found several examples of misconceptions in published literature. Clarification on the definition and goals of human factors in health care was needed. The panel members recognized this need and began to prepare a summary of five basic human factors concepts, with the goal of bridging the gap between health care and human factors communities.
The authors outlined the following five basic concepts about human factors. An understanding of these five fundamental human factors concepts opens the door to meaningful collaboration between human factors and health care professionals to improve systems of care.
-
#1: "Human factors is about designing systems that are resilient to unanticipated events."
- Everyone makes mistakes. It is part of our human experience. Human factors experts gather scientific data about how people think and work to understand how they interact within a system. Then they can help design systems that support people and their work. More resilient system designs help mitigate the effects of mistakes and errors that do occur.
-
#2: "Human factors addresses problems by modifying the design of the system to better aid people."
- There are plenty of poorly designed systems at work. Most people think about how to make people change to fit into those systems, but human factors experts face work challenges differently. They look at what is wrong with systems and change things like technology, processes or tools so the design of the system improves to help patients, providers and caregivers. Improving system design to better support people is a more effective strategy than expecting people to change their behavior and adapt to poor design.
-
#3: "Human factors work ranges from the individual to the organizational level."
- Human factors experts also look at how organizations are designed, including their policies and procedures, so that organizational level components can be better designed and coordinated to aid people's work. Health care professionals work in very complex environments; understanding the broader organizational influences on an individual's work is often necessary to ensure effective design of health care systems.
-
#4: "Human factors is a scientific discipline that requires years of training; most human factors professionals hold relevant graduate degrees."
- Some human factors methods like interviewing or observing people may seem simple, but it takes intensive training and experience to learn and correctly apply human factors scientific theory and methods. When human factors and health care experts work together, this creates an environment for substantive improvements in safety and effectiveness of care.
-
#5: "Human factors professionals are bound together by the common goal of improving design for human use, but represent different specialty areas and methodological skills sets."
- Human factors training is most often rooted in engineering and psychology programs, however, most human factors experts specialize in a focus area that consists of particular knowledge and methods. It is important to identify human factors specialty areas that fit with an organization's or project's goals and seek experts that can bring the requisite skill sets to health care improvement.
Dr. Russ and her co-authors summarize a very large body of information and offer many insights to anyone wanting to improve health care quality, efficiency, or safety.
View the Open Access article for complete details.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
"Flipping" Health Care Professionals’ Way of Thinking about Patient Safety: An interview with Dr. John Gosbee
Christopher Petteys, MBA, Program Coordinator, Human Factors Engineering and
Linda C Williams, Program Specialist, RN, MSI, VA National Center for Patient Safety
From 1999 to 2006, Dr. John Gosbee worked at VA's National Center for Patient Safety (NCPS). During his time with NCPS, he led the development of patient safety and Human Factors Engineering residency and medical school curriculum. He also led the Human Factors Engineering analysis of adverse events and close calls involving medical devices and software, including as the liaison to companies to rectify design issues. Dr. Gosbee originally trained as a physician at Wright State University, which is considered a cradle of Human Factors Engineering. He eventually realized the program would be important in his career in Aerospace Medicine. Dr. Gosbee worked for four years at National Aeronautics and Space Administration (NASA) after his residency. Dr. Gosbee currently runs a Human Factors Engineering and health care consulting firm and leads residency patient safety activities at the University of Michigan Health System. His background is a unique blend of both clinical and human factors training including Aviation Human Factors.
- 1. What is your role with VA?
- My role with VA can be traced back to 1999 to 2006 at the NCPS. Additionally, toward the end I spent a lot of time with the Office of Information Technology tracking down problems that occurred with VA health information technology and related computer systems. I also worked with various universities across the country teaching Human Factors Engineering and interacting with a variety of committees and folks writing human factors related test questions for medical students taking board exams. My VA connection continues through participation in a variety of different types of committees. For example, the Food and Drug Administration, as they try to strengthen their Human Factors Engineering activities, has involved me as they apply human factors standards and guidelines in the support of redesign and evaluation of medical devices pre and post marketing. This is very similar to what happens with VA systems, so in that respect you find an overlap.
- 2. Describe your role in establishing the NCPS.
- My role can be broken into three parts that were somewhat related. The first, Human Factors Engineering, involved teaching the basic science behind patient safety to over 3000 VA employees over the years. In this regard, we were like an educational outreach organization to the various VA facilities. The second piece had to do with acting as an internal consultant for VA facilities to help them understand the human factors aspects of root cause analyses and patient safety. The third piece had to do with creating and developing a Human Factors Engineering based curriculum to help guide medical schools and residency programs to think differently on how they trained doctors. 50 percent of all doctors have a portion of their training in a VA medical center. That means that doctors in training, residents, potentially have a large role in patient safety in VA medical centers. So we created a Human Factors Engineering based curriculum that enables educators to think differently about how they teach their doctors in training. This also gives residents a larger role in creating and sustaining safe systems in VA health care delivery.
- 3. What other institutions or organizations do you work for?
- My thought process for my career was to think of ways to improve the health care system--the people, the staff, and the medical devices. My time is now split between working with universities to change the curriculum for medical students to include patient safety and Human Factors Engineering and consulting with companies developing and designing medical devices. I also help teach the Systems Engineering Improvement in Patient Safety (SEIPS) course at the University of Wisconsin that a lot of VA employees seem to attend, as well as Human Factors Engineering and patient safety courses at other universities.
- 4. How were you introduced to the concept of Human Factors Engineering?
- I had wanted to do medicine but I didn't love it enough to spend eighty to one hundred hours on it weekly. I looked for alternatives to traditional residencies and gradually made my way to an Aerospace Medicine residency at Wright State University, which also happened to be a cradle of Human Factors Engineering. Human Factors Engineering is a discipline I stumbled upon with a chance meeting of Anthony J. Cacciopo, PhD., who was serving as chair of a Human Factors Engineering program he just started at the University. By this point, I had developed enough interest to realize that Human Factors Engineering was going to be useful in pursuing my career in Aerospace Medicine. After I finished my residency, I worked for four years at NASA. We used simulation and Human Factors Engineering to build systems, for example, we worked on a space hospital.
- 5. Is there anyone in particular who you deem influential or anyone you influenced?
- People don't want to give up the notion that they have control and can avoid making mistakes. When it comes to influencing health care workers, it takes a 180 degree brain flip for them. If you aren't successful in provoking the brain flip, in getting people to think in another direction, the lack of influence can be really astounding. If the flip doesn't occur, no amount of screaming at people will bring about change. For this reason, the learning is necessarily attitudinal and emotionally based. If they understand the basic principles of Human Factors Engineering, their world perspective is flipped in a way that they never see their work environment in the same way again.
Terry Fairbanks, MD, MS is a name that comes up as someone who has had a large impact in the field of Human Factors Engineering. Terry talked with me when he first set out to pursue medicine and human factors and he is now making strides in the field. He is currently the Director of the National Center for Human Factors Engineering in Health Care.
Jeff Cooper, PhD, is someone who has influenced me and he ended up writing the forward to the book my wife and I wrote in 2005, "Using Human Factors Engineering to Improve Patient Safety". Jeff is currently a Professor of Anesthesiology at Harvard Medical School.
- 6. How do you use/employ human factors in your work?
- I teach and help implement Human Factors Engineering in companies trying to change their product development process for medical devices and systems. I also teach Human Factors Engineering to health care organizations and universities at many levels and to a variety of professions. I teach using the Human Factors Engineering method of usability testing to help them be surprised at what they can find. Their discoveries motivate the use of the same methods in their work. It's much easier to have them see someone not read the directions on a life-saving device while trying to save their friend rather than lecturing, "People don't read directions." Putting them in a situation of seeing that seems to get more mileage.
- 7. What Human Factors – based project do you feel made the biggest impact in VA? Why?
- The introduction of Human Factors Engineering has been
 impactful in the way that it enhances patient safety especially since VA is affiliated with universities and residency programs. The Accreditation Council for Graduate Medical Education (ACGME) is the monitoring/regulatory agency for residencies, conducting regular surveys to ensure compliance to applicable standards, including human factors standards. Loss of accreditation became a penalty that was handed out if the guidelines were not adhered to. Before I left VA, we also had an opportunity to re-evaluate our faculty development curriculum workshops, comparing outcomes in order to measure effectiveness and gauge positive correlations. Over time, a lot of universities, I think, were surprised to find VA educators in their VA–affiliated medical centers were way out ahead and actually had residents and others involved in patent safety and human factors-based projects for quite some time. impactful in the way that it enhances patient safety especially since VA is affiliated with universities and residency programs. The Accreditation Council for Graduate Medical Education (ACGME) is the monitoring/regulatory agency for residencies, conducting regular surveys to ensure compliance to applicable standards, including human factors standards. Loss of accreditation became a penalty that was handed out if the guidelines were not adhered to. Before I left VA, we also had an opportunity to re-evaluate our faculty development curriculum workshops, comparing outcomes in order to measure effectiveness and gauge positive correlations. Over time, a lot of universities, I think, were surprised to find VA educators in their VA–affiliated medical centers were way out ahead and actually had residents and others involved in patent safety and human factors-based projects for quite some time.
- 8. Where do you see the greatest potential for the application of human factors principles in VHA?
- The greatest potential is in selecting and building systems with the fewest Human Factors Engineering design flaws and continuing to teach clinicians. That is, we need to continue to influence and teach residents and medical students, and help them develop a 'systems' way of thinking. We also need to continue to apply Human Factors Engineering to the various computer systems, especially in chronic or ambulatory care. Having a human factors mindset and the tools for chronic care and home care is essential to reducing readmissions and other goals of patient centered care.
- 9. Have you seen changes in the interest in or awareness of human factors in VA? What are they?
- In recent times I have seen a lot of VA staff attending sessions at the SEIPS course at the University of Wisconsin, as well as at the annual Human Factors and Ergonomics Society Symposium on Human Factors and Ergonomics in Health Care. This is an indication that human factors awareness is rising in VA.
- 10. What are the most troubling/difficult challenges to the application of Human Factors Engineering in health care?
- If you are incorporating human factors elements into frontline patient safety, you have to learn to deflect people's resistance in a positive way. Mindset change is crucial and as we say, we need to flip the brain 180 degrees because without that change in perspective, people tend to resort to writing or revising policies and making more rules in their efforts to solve problems; rather than addressing the design issues at the heart of the problem.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Workarounds Illuminate Gaps in the EHR
Jason J. Saleem, PhD, Technical Information Specialist, Human Factors Engineering, Office of Informatics and Analytics
Workarounds are nonstandard procedures that people develop because of real or perceived limitations in system or workflow design. Over the last several years, my colleagues and I have investigated HIT workarounds from a Human Factors Engineering perspective. Human Factors Engineering seeks to design systems that maximize human cognitive and physical capabilities and minimize our limitations. By using a Human Factors Engineering perspective, the goal is to design or redesign a system to support human capabilities and limitations rather than trying to make a person adapt to suboptimal design. Otherwise, people develop workarounds to support their work over time when the system fails to do so.
Our initial work focused on paper-based workarounds to the EHR and later expanded to computer-based workarounds as well (e.g., using a software program in a way it wasn't intended to be used to support clinical work). We performed a pilot study on workarounds to VA's current EHR, the Computerized Patient Record System (CPRS), then focused on workarounds involving computerized consult management, and expanded our findings to other major benchmark institutions outside of VA. Our objective was to understand reasons why health care workers develop workarounds. Understanding these different types of workarounds provides a foundation for EHR innovation to better support the needs and workflow patterns of clinicians.
In our work, we found several distinct categories of paper- and 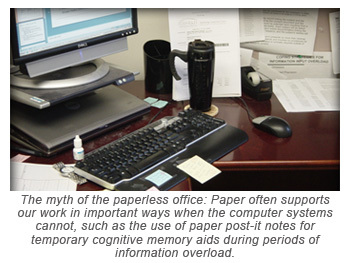 computer-based workarounds to the system's designers and implementers envisioned use of the EHR. In our studies, the most frequent reasons for using paper workarounds were for efficiency and ease of use. The second most frequent reason was as a memory aid (i.e., paper often served an important and necessary cognitive memory aid). The third most frequent reason was to recognize or alert others to new or important information. Another common reason related to sensorimotor preferences is participants described a preference for the following: mobility of the artifact; ability to hear something; hold something tangible; something concrete to deliver; and/or work with something that can be easily manipulated (e.g., hand notes). Additional categories uncovered in the studies were: awareness (directing someone's attention to specific, new information); task specificity and need for customization; task complexity (the demands of the task require more than the capabilities of CPRS); data organization and display; longitudinal data processes; trust; security; and the lack of a correct path for executing the tasks in CPRS. computer-based workarounds to the system's designers and implementers envisioned use of the EHR. In our studies, the most frequent reasons for using paper workarounds were for efficiency and ease of use. The second most frequent reason was as a memory aid (i.e., paper often served an important and necessary cognitive memory aid). The third most frequent reason was to recognize or alert others to new or important information. Another common reason related to sensorimotor preferences is participants described a preference for the following: mobility of the artifact; ability to hear something; hold something tangible; something concrete to deliver; and/or work with something that can be easily manipulated (e.g., hand notes). Additional categories uncovered in the studies were: awareness (directing someone's attention to specific, new information); task specificity and need for customization; task complexity (the demands of the task require more than the capabilities of CPRS); data organization and display; longitudinal data processes; trust; security; and the lack of a correct path for executing the tasks in CPRS.
Some of the paper- and computer-based workarounds revealed were problematic. Circumventing EHRs via paper or electronic tools introduces the potential for gaps in documentation as well as the unintentional propagation of errors. However, some of the same workarounds offered efficiencies and other advantages over the "standard" electronic workflows, and disclosed potential limitations of the design of the computerized systems. Workarounds can also sometimes reflect the resiliency and ingenuity of people to find ways to work past EHR limitations to provide quality care. Therefore, a well-designed EHR should support the use of important paper supplementation or alternative computer workflows while minimizing the potential for gaps in EHR documentation.
In a recent case at a VA medical center (unrelated to our studies), an Emergency Department (ED) nurse used the EHR to document a patient allergy to aspirin. A physician later bypassed the EHR and hand-wrote an order for an anti-inflammatory drug that is contraindicated for aspirin (VA OIG Report No. 13-00505-348). This same example of an "efficiency" workaround using paper orders in the ED was documented in our previous study. Had the physician order been entered into the EHR, a drug alert would have automatically been generated to warn the physician of the allergy. The adverse event that followed was preventable. However, the use of such a workaround does suggest that there are times when an ED physician needs to be able to efficiently input an order "on the go" in an emergency situation without being tethered to a workstation. Nevertheless, a hand-written order creates a gap or delay in EHR documentation. Perhaps this case points to a greater need to adopt advanced mobile technologies or better integrate existing technologies into clinical workflow.
Although the term "workaround" has a negative connotation and can even create paths to medical error, it is better viewed as a neutral term. Many of the alternative workflows and tools revealed by our studies genuinely supported the clinicians in their work in important ways where the EHR could not. Workarounds are often a reflection on the system and its limitations and they give us ideas on how to improve the interface between the health care provider and the EHR. When a workaround cannot be eliminated through enhanced EHR design, then paper and computer-workarounds need to be well-coordinated with the EHR to prevent gaps in documentation and the potential for medical error.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Health Care Human Factors Curriculum: Improving Patient Safety by Making Human Factors Engineering Accessible
Kristen Miller, DrPH, MSPH, Research Fellow, VA NCPS,
Tandi Bagian, MSE, Director, Human Factors Engineering Division, VA NCPS
Preventable or avoidable adverse events can often be attributed to a failure to follow recognized, evidence-based best practices or guidelines at the individual and/or system level. Studies of adverse patient incidents have heightened our awareness of the benefits of re-engineering systems and processes to reduce or prevent use-errors. The time has come for organizations to apply the very same cognitive ergonomics and human factors analyses we expect of device manufacturers to make health care services safer for patients. The re-engineering of processes combined with a shift to a culture of safety is essential if health care organizations are to continue to reduce harm to patients from increasingly complex medical procedures and associated use-error. Health care facilities often struggle in their ability to standardize approaches and decrease complexity, yet it is relatively straightforward to reap organizational benefit from incorporating an awareness of and an appreciation for Human Factors Engineering.
Despite the existence of considerable information about how to improve care through the application of Human Factors Engineering, health care professionals are not provided a means to ensure sufficient education in health care human factors and the associated impact on patient safety. Additionally, even when existing information is taught, providers are challenged to translate and apply knowledge to effect safe patient care. VA's NCPS Health Care Human Factors Modules were designed to address these challenges by combining dissemination of existing knowledge and recent research into accessible, hands-on activities that drive home human factors and patient safety competencies. These modules represent an innovative and engaging way to allow providers and administrators alike the ability to advance the shift to systems thinking through high-impact education.
The Health Care Human Factors Modules represent an accessible, novel approach to equip the future instructor  with foundational knowledge necessary to understand the context, key principles, and competencies associated with health care human factors, and how these tenets and skills are applied in patient safety. Future instructors may be clinical, administrative, or executive professionals or other individuals who have a role in implementing patient safety practices or other improvement projects in their health care communities. Rather than creating a curriculum that targets one specific health care profession, the goal of the project is to develop modules that can be taught to interested staff at individual facilities, broadening the utility of the project as a whole. The goals are to provide learners with the requisite knowledge, skills, behaviors, and attitudes to understand the issues involved in safe patient care, and also to be able to use Human Factors Engineering methods to identify and mitigate patient safety hazards in their health care setting. with foundational knowledge necessary to understand the context, key principles, and competencies associated with health care human factors, and how these tenets and skills are applied in patient safety. Future instructors may be clinical, administrative, or executive professionals or other individuals who have a role in implementing patient safety practices or other improvement projects in their health care communities. Rather than creating a curriculum that targets one specific health care profession, the goal of the project is to develop modules that can be taught to interested staff at individual facilities, broadening the utility of the project as a whole. The goals are to provide learners with the requisite knowledge, skills, behaviors, and attitudes to understand the issues involved in safe patient care, and also to be able to use Human Factors Engineering methods to identify and mitigate patient safety hazards in their health care setting.
The core curriculum represents an important body of work with essential knowledge about human factors and patient safety and brings participants up to speed with regards to recent practices and innovative interventions. The first set of plenary modules is designed to cover fundamental human factors and patient safety topics including health care ergonomics, cognition, usability, proactive risk assessment, and root cause analysis. A middle group of modules progresses to specific topics including stress and fatigue, teamwork and communication, and multitasking and mitigating interruptions. The final set of modules will be created based on participant input and hot topics in the field.
Hands-on activities through simulation are a key component to Human Factors Health Care Curriculum. David Gaba defines simulation as "a technique – not a technology – to replace or amplify real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner (2004). Rather than hope the engineering tools and strategies make sense to health care professionals, basic principles and a variety of human factors tools are discussed and demonstrated through hands-on lab activities using both 'every day' and health care examples. In some instances, the activities use non-health care themes to draw parallels between familiar concepts and health care. In other instances, health care simulation activities provide an opportunity to empower and equip learners for future scenarios. Practice scenarios can help learners develop effective communication techniques or re-enact the circumstances of past adverse events to highlight the importance of speaking up within a care team.
In the fall of 2013, VA NCPS Health Care Human Factors Modules were piloted preceding rollout in VA facilities. Based on quantitative evaluation and qualitative responses from participants, the pilot trial of the modules successfully demonstrated that participants acquired Human Factors Engineering knowledge that will be applied in their current day-to-day operations and in future health care endeavors. Participants thought that activities encouraged creative thinking and engaged participants in learning. Post course surveys consistently indicate participants find the course worthwhile. Through the various scenarios, participants can readily see how individual limitations and system vulnerabilities may compromise patient outcomes and/or contribute to occupational injury. VA's experience shows that once organizational members believe they can perceive and evaluate vulnerabilities in their system, they begin to realize the actions they can take to reduce or eliminate vulnerabilities. Ultimately, the Veteran patient is the beneficiary as health care vulnerabilities are addressed.
As the modules move forward through pilot, roll-out, and evaluation, NCPS aims to bring health care human factors and patient safety to the point of sustainability – being owned in various clinical settings. The paramount objective of these modules is for providers and administrators alike to learn health care human factors and key patient safety practices, and put them into action in their immediate areas of responsibility for patients. VA's NCPS Health Care Human Factors Modules will not only provide a core curriculum but a 'human factored' framework for the ongoing education and training of health care professionals. VA NCPS Health Care Human Factors Modules are designed to forge partnerships between human factors and clinical experts for successful long-term collaborations, as well as redesign and implementation of health care processes for improved safety and effectiveness.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
|

 Mobile App Design Brief: Navigation Bar Design Considerations Mobile App Design Brief: Navigation Bar Design Considerations
Donna Harrigan, BA, Management and Program Analyst, Human Factors Engineering, Office of Informatics and Analytics
The new Mobile App Design "brief" series will highlight best practices in action in VA for mobile UI design certifications. This first brief focuses on navigation bar design.
Who likes intuitive, easy to use apps? I'll venture out on a limb and say, we all do! UI's that  are built from user experience best practices, and industry guidelines and standards, provide a familiar model for a user with regard to an application's appearance and behavior. This holds true when navigating through an application. are built from user experience best practices, and industry guidelines and standards, provide a familiar model for a user with regard to an application's appearance and behavior. This holds true when navigating through an application.
Users are familiar with the navigation bar being located at the top of an application screen, just below the status bar. When designing  the look of a customized navigation bar for a mobile application, it is wise to adhere to the device operating system guidelines. For example when constructing the back button, use the chevron symbol accustomed for iOS* and android apps and position it to appear in the left end of the bar. The image in Figure 2 is a navigation bar from the iOS 7 Human Interface Guidelines and depicts the best practice mentioned above. the look of a customized navigation bar for a mobile application, it is wise to adhere to the device operating system guidelines. For example when constructing the back button, use the chevron symbol accustomed for iOS* and android apps and position it to appear in the left end of the bar. The image in Figure 2 is a navigation bar from the iOS 7 Human Interface Guidelines and depicts the best practice mentioned above.
Mental health professionals in VA developed the "Moving Forward" mobile application featured in the image to the left and adheres to both iOS guidelines and VHA UI Design Certification criteria. Notice the consistency of the navigation bar with the user experience best practices, such as button shapes ("Back" and "Favorites" buttons), inclusion of the screen title and spacious placement of controls.
When button shapes mean the same thing on all screens within the application and there is consistency in behavior, the app is easier to use. In sum, avoid making your users learn a new way of performing a function when there are tried and true best practices available!
*Apple® mobile operating system
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
|
