Having trouble viewing this email? View it as a Web page.
 |
 In this issue of the newsletter, we present an article about a knowledge repository created to facilitate VA's adoption and institutionalization of Human Factors Engineering for the development of health information technology (HIT) systems. Article two describes a color-coding system for back-table medications, which will enhance recognition of high-risk medications to reduce the likelihood of inadvertent misadministration. In the third article, an interview with Dr. Danielle Hoover demonstrates enhanced patient safety, a major objective of human factors engineering. The fourth article shows eye tracking and computer mouse activity being used to measure clinicians' cognitive workload. The final article outlines workflow modeling methods providing foundational understanding of a clinical work process to support HIT human-technology integration considerations. We also continue our feature on Mobile Application Design and welcome your feedback, which can be submitted to VHA10P2HFQ@va.gov. In this issue of the newsletter, we present an article about a knowledge repository created to facilitate VA's adoption and institutionalization of Human Factors Engineering for the development of health information technology (HIT) systems. Article two describes a color-coding system for back-table medications, which will enhance recognition of high-risk medications to reduce the likelihood of inadvertent misadministration. In the third article, an interview with Dr. Danielle Hoover demonstrates enhanced patient safety, a major objective of human factors engineering. The fourth article shows eye tracking and computer mouse activity being used to measure clinicians' cognitive workload. The final article outlines workflow modeling methods providing foundational understanding of a clinical work process to support HIT human-technology integration considerations. We also continue our feature on Mobile Application Design and welcome your feedback, which can be submitted to VHA10P2HFQ@va.gov.
- Jason J. Saleem, PhD, Editor-in-Chief.
|
|
| |
|
 |
 |
Facilitating VA's Adoption of Human Factors Engineering: Knowledge Sharing
Ross Speir, Program Manager, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics, Ben D. Harper, MS., Human Factors Engineer, OIA Human Factors Engineering, Ann M. Pennington, Senior Human Factors Engineer, OIA Human Factors Engineering
In the 2012 Spring issue of the Human Factors Quarterly, Ross Speir argued that designing next generation Health Information Technology (HIT) systems for the VA would require project teams to put user experience at the center of system development. The article described how focusing on the end user experiences throughout the development lifecycle would ensure that VA systems enable users to carry out clinical work efficiently and effectively. In the two years since the article was published, many...
Read More >
|
- Upcoming Events
-
HFES Annual Meeting, October 27-31, Chicago, IL
-
AMIA Annual Symposium, November 15-19, Washington, D.C.
- Informational Links
- Human Factors Engineering (HFE) within the Veterans Health Administration (VHA) Office of Informatics and Analytics, Health Informatics Division seeks to increase awareness of human factors products and services among clinical end-users and other stakeholder groups. This quarterly newsletter serves to engage these communities in shared communication and collaboration around human factors-related issues.
Access and review previous issues of this newsletter
- Editor-in-Chief:
- Jason J. Saleem, PhD, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Managing Editor:
- Christopher Petteys, MBA, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics
- Editorial Board Members:
- Michael W. Smith, PhD, Houston VA HSR&D Center for Innovations
- Rachel Wiebe, RD, CPHQ, Health Solutions Management, Health Informatics, Office of Informatics and Analytics
- Linda C Williams, RN, MSI, VA National Center for Patient Safety
- Scott D. Wood, PhD, Informatics Patient Safety, Office of Informatics and Analytics
|
 |
 |
Standardized Color-Coding Back Table Solution
Linda Cicconi RN, BSN, CNOR - OR, Quality Manager, David Eibling, MD, Chief of Otolaryngology, Michael Mangione, MD, Chief of Anesthesiology, VA Pittsburgh Healthcare System
Unidentified "back-table" medications used in the operating room have been flagged as a major threat to patient safety. "Back table" medications are readily available and accessible in the sterile field of the operating room. These are common injectable solutions that may need to be used during the operation and in some cases during an emergency. The requirement that solutions on the sterile field be labeled to prevent misadministration is a standard in all operating rooms. In order to assure standardization with other medications used in...
Read More >
|
|
|
 |
The Intersection of Human Factors Engineering and Patient Safety:
An Interview with Dr. Danielle Hoover
Scott D. Wood, PhD, Health Systems Specialist, Informatics Patient Safety, Office of Informatics and Analytics
Dr. Danielle Hoover, M.D., MPH is Board Certified in Internal Medicine and Clinical Informatics, and provides Primary Care to Veterans in Ann Arbor, Michigan.
What is your role with VA?
I work in the VA National Center for Patient Safety (NCPS) as part of the Human Factors Engineering team. The team is comprised of biomedical engineers, physicians and the product recall office. We represent the end user from a patient safety standpoint. My goal is to bridge organizational gaps and to ensure clear communications between the engineers, clinicians and...
Read More >
|
|
|
 |
Can Eye Tracking and Electronic Health Record Mouse Activity Tell us when Clinicians are Overloaded?
[1] Alan Calvitti, PhD [2] Nadir Weibel, PhD [3] Harry Hochheiser, PhD [4] Lin Liu, PhD [5] Kai Zheng, PhD [6] Charlene Weir, PhD [7] Shazia Ashfaq, MD, MBA [8] Steven Rick, BS [9] Zia Agha, MD, MS [10] Barbara Gray, MA [11] Colleen Emmenegger, MS
The amount of thought and attention needed to complete complicated tasks – known as “cognitive load” – can have an impact on physicians’ ability to accomplish important tasks with electronic health records (EHRs). To better understand when physicians experience cognitive load, we are conducting an ongoing usability study of VA’s EHR, the Computerized Patient Record System (CPRS). Based at VA San Diego, this study focuses on clinicians’ cognitive load during outpatient visits. We are...
Read More >
|
|
|
 |
Gaining Value from Baseline Business Process Modeling
Brad Branham, Supporting Analyst / Project Lead, Office of Quality, Safety, and Value (QSV), Product Effectiveness; Ferenc Ayer, Program Manager, QSV, Product Effectiveness
Business process modeling (BPM), or workflow mapping, provides an organization with a mechanism to understand its processes through different aspects (such as user roles, technology enablers, or governing statements) and in turn, activities from which the organization derives value. The development of a business process model is a fundamental starting point as it provides the "context" within which all process management and improvement is carried out. BPM can...
Read More >
|
|
|
 |
Mobile Application Design Brief:
Cognitive Load
Donna Harrigan, BA, Management and Program Analyst, HFE, Health Informatics Division, Office of Informatics and Analytics
In previous issues of this newsletter, I've written about user interface (UI) design standards and best practices such as the use of simplicity and minimal design to highlight key information on a page and consistency in navigation and terminology to provide familiarity for a user. The common goal is to make it easier for a user to get the information needed to perform a task or make a decision. An app should be designed so the user can effortlessly comprehend the...
Read More >
|
| |
Back to top of article summary | Back to top of newsletter
|
|
Facilitating VA's Adoption of Human Factors Engineering: Knowledge Sharing
Ross Speir, Program Manager, Human Factors Engineering, Health Informatics, Office of Informatics and Analytics, Ben D. Harper, MS., Human Factors Engineer, OIA Human Factors Engineering, Ann M. Pennington, Senior Human Factors Engineer, OIA Human Factors Engineering
In the 2012 Spring issue of the Human Factors Quarterly, Ross Speir argued that designing next generation Health Information Technology (HIT) systems for VA would require project teams to put user experience at the center of system development. The article described how focusing on the end user experiences throughout the development lifecycle would ensure that VA systems enable users to carry out clinical work efficiently and effectively. In the two years since the article was published, many VA HIT development teams have successfully adopted user-centered practices to improve the “user experience (PDF).” In this article we will introduce a knowledge repository that was created to capture and share the practices of user-centered design in VA.
The Human Factors Body of Knowledge (HF BoK) is an information repository meant to promote VA's adoption of user-centered practices. This repository is an organizational resource that provides project teams with proven methods and guidelines for putting end users at the center of system requirements gathering, design, development, testing, procurement, and implementation. Information in the HF BoK is collected from several sources, both within and outside VA, to achieve three primary objectives.
The first objective of the HF BoK is to reduce redundancies and duplicative work in the practice of human factors engineering. To this end, the HF BoK publishes all of the findings from work carried out by OIA Human Factors Engineering. Currently, reports from over 100 human factors studies are available in the HF BoK; these include user research studies, user interface design work, and usability test results of VA HIT systems. These reports allow project teams to leverage information collected by previous project teams.
The second objective is to promote adherence to industry and government standards related to HIT design and testing organizations such as the National Institute of Standards and Technology (NIST) and the International Organization for Standardization (ISO) have published robust and detailed standards on various topics related to human factors engineering; and the HF BoK includes user-centered design standards, user interface design standards, usability testing methods, and standards for validating HIT system usability. Project teams are encouraged to utilize these standards in the HF BoK in order to follow evidence-based best practices.
The third objective of the HF BoK is to help bridge the gap between human factors research and VA practice. Research articles and researcher presentations are continually added to the HF BoK to support VA's utilization of evidence-based practices for designing usable HIT systems.
Information from these sources is organized in the HF BoK to serve as a knowledge repository for VA HIT project teams. Below are examples of content that has been developed or is currently in development:
- Human Factors Methods that help project teams understand the services provided by HFE at different phases of the development lifecycle to help improve usability. Method descriptions include the purpose of the method, timeframe, dependencies required to execute the method, expected outcomes and limitations. VA has executed each of these methods to support HIT design, development, and testing. Lessons learned are collected to improve method effectiveness and efficiency.
- User Interface Design Patterns from industry and research, and practiced within VA to support the reuse of evidence-based designs across VA HIT systems.
- User Personas developed from HIT projects and from data on clinician and Veteran populations provide project teams with a better understanding of various users and their work environments.
- Sample language for VA contracts provides guidance on obtaining contract support for user-centered design or usability testing for HIT development or Commercial Off-the-Shelf (COTS) procurement projects.
The HF BoK is meant to serve as VHA's institutional knowledge repository of human factors engineering as it is practiced for the design, testing, procurement, and implementation of VA HIT systems. This repository will serve to hasten the organization's adoption of human factors engineering practices that are needed to support next generation HIT system development. To learn more about the HF BoK, visit the site and browse the growing content, or contribute your own content. For the HF BoK to realize its full potential, feedback and guidance is needed from the VHA community.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Standardized Color-Coding Back Table Solution
Linda Cicconi RN, BSN, CNOR - OR, Quality Manager, David Eibling, MD, Chief of Otolaryngology, Michael Mangione, MD, Chief of Anesthesiology, VA Pittsburgh Healthcare System
Unidentified “back-table” medications used in the operating room have been flagged as a major threat to patient safety. "Back table" medications are readily available and accessible in the sterile field of the operating room. These are common injectable solutions that may need to be used during the operation and in some cases during an emergency. The requirement that solutions on the sterile field be labeled to prevent misadministration is a standard in all operating rooms. In order to assure standardization with other medications used in the operating room, we adopted a system of pre-printed labels that adopts the International Organization for Standardization (ISO) standard used for injectable anesthesia medications. This labeling typically consists of a white label with dark lettering applied by the scrub nurse, and we have postulated that a color-coded medication labeling system might potentially enhance scrub nurse recognition of labeled solutions.
Inadvertent injection of misidentified solutions on the sterile field is a rare but potentially catastrophic error. Occasionally these errors have led to intra-operative deaths that have received widespread publicity, such as the death of Bob East, an award winning photographer for the Miami Herald in 1985, following instillation of unlabeled glutaraldehyde into his spinal drain. Ten years later, 7 year old Ben Kolb died due to the inadvertent injection of concentrated 1:1000 epinephrine while undergoing routine ear surgery. Shah and coauthors pointed out that the necessity for both injectable lidocaine containing 1:100,000 epinephrine and concentrated topical 1:1000 epinephrine to be present on the back table in the same surgical procedure sets the stage for inadvertent injection of concentrated epinephrine. A 2012 Patient Safety Alert by VA National Center for Patient Safety identified the risk of inadvertent injection of concentrated epinephrine intended for topical use.
A prior study demonstrated that the accuracy of back-table medication labeling is improved when preprinted labels are provided. Although it is intuitive that color-coded labels would aid in medication recognition, experience in other health care settings suggests otherwise due to lack of standardization. For example, non-standardized color-coded wrist bands have led to adverse outcomes when health care workers base interventions (or lack thereof) on the presence of wrist bands obtained elsewhere for other purposes.
Two notable exceptions to this lack of standardization exist in healthcare. Topical ophthalmologic medications are color-coded per an industry-wide standard, as are injectable medications used by anesthesiologists. The anesthesia color-coding system has been in use for 25 years, and in 2008 was assigned an ISO standard, 26825:2008. All anesthesia personnel as well as manufacturers are aware of the protocol.
Interestingly, a simulator-based study presented at the 2008 meeting of the American Society of Anesthesiologists(ASA) demonstrated that color-coding injectable medications had no measureable benefit in “normal” situations. However, in simulated high stress situations, utilization of color-coded medications increased speed and accuracy of drug administration.
We based our intervention on these two studies and reasoned that keeping the color-coding system congruent with the ISO standard would increase recognition and enhance learning.
Team members consisting of representatives from anesthesia, surgery, operating room, and pharmacy reviewed and revised proofs. The workgroup coordinated with specific services to assure that all necessary labels would be available for any procedure performed by each specific surgical specialties area.
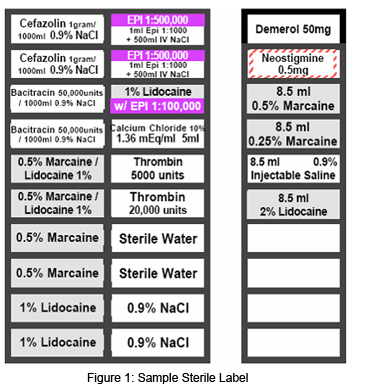 Preprinted labels were purchased and packaged for 12 specialty areas, including General Surgery, Genito-Urinary/Kidney, Transplant, Gynecology, Liver Transplant, Neurosurgery, Open Heart, Ophthalmology, Orthopedics/Spine/ Podiatry, Otorhinolaryngology (ENT), Plastics, Thoracic, and Vascular. Figure 1depicts an example of one such set. Preprinted labels were purchased and packaged for 12 specialty areas, including General Surgery, Genito-Urinary/Kidney, Transplant, Gynecology, Liver Transplant, Neurosurgery, Open Heart, Ophthalmology, Orthopedics/Spine/ Podiatry, Otorhinolaryngology (ENT), Plastics, Thoracic, and Vascular. Figure 1depicts an example of one such set.
At this time, we have no data to confirm that this innovation has resulted in substantive changes due to the very rare occurrence of such events. It is important to note that the introduction of color-coded labels impacts only a single step in the process of back-table medication selection and administration. Attention to established policies and procedures regarding back-table medications is an expectation of all operating room personnel. Awareness of the inherent risks of mis-labeling and mis-administration of back-table medications can assist in maintaining vigilance; an awareness that can be reinforced via frequent Operating Room (OR) team discussions.
For example, VA Pittsburgh Healthcare System (VAPHS) OR policy was revised to mandate the use of the preprinted labels and add the requirement that high risk medications, such as 1:1000 topical epinephrine, be tinted with dye. Modification of labels to enhance accuracy, such as designation of oxymetazoline as a high risk sympathomimetic, as well as monitoring of compliance remains an ongoing process at VAPHS to enhance patient safety.
We postulate that the adoption of an established color-coding system for back-table medications in the OR setting may enhance recognition of high risk medications and reduce the likelihood of inadvertent misadministration. Future testing of our intervention is needed, such as in a simulated OR environment, to assess if the adoption of color-coded medication labeling for use on the sterile field in the OR may be of benefit in reducing the likelihood of selecting the incorrect solution.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
The Intersection of Human Factors Engineering and Patient Safety: An Interview with Dr. Danielle Hoover
An Interview with Dr. Danielle Hoover
Scott D. Wood, PhD, Health Systems Specialist, Informatics Patient Safety, Office of Informatics and Analytics
Dr. Danielle Hoover, M.D., MPH is Board Certified in Internal Medicine and Clinical Informatics, and provides Primary Care to Veterans in Ann Arbor, Michigan.
- What is your role with VA?
- I work in the VA National Center for Patient Safety (NCPS) as part of the Human Factors Engineering team. The team is comprised of biomedical engineers, physicians and the product recall office. We represent the end user from a patient safety standpoint. My goal is to bridge organizational gaps and to ensure clear communications between the engineers, clinicians and those involved in informatics at the local facility and Central Office levels.
- How were you introduced to the concept of human factors?
- In 2007, I joined VA as a National Quality Scholars Fellow in Cleveland. During orientation, we attended a presentation by NCPS staff which included an overview of patient safety and included information on Human Factors Engineering. I had never heard that term before, nor had I ever considered a medical device or procedure as good or bad from a design perspective. For instance, we looked at pictures of pleural drainage tubes. The tubes were identical in appearance, but functioned differently. It was easy to see how this design flaw could result in the wrong tube being mistakenly connected to drain a cavity, preventing proper healing. This approach made so much sense that I began applying this same process to systems design. I transferred the human factors principles I had learned over to my every day use, such as making medication lists easier to read for patients and providers.
- How do you use or employ human factors in your work?
- At NCPS we receive safety reports and root cause analyses when actual harm or a near miss event occurred to a patient.
 Our job is to review the reports and determine how best to prevent the problem from recurring. We look at the facility's processes and systems as a whole to determine where safety measures can be implemented to prevent further harm. Sometimes the facility is attempting to address the problem from a single point of view. We take a systems approach by considering the point of view of the end user and others from the organization, such as the biomedical engineer, the clinician, and the support staff. Figure 2 shows the cross pollination of information and problem perception in an effort to raise the varying areas' awareness and understanding of each other's perspectives when addressing issues. For example, we received a report of a medical device on a computer workstation that was timing-out during a procedure that can take up to 120 minutes. The facility, assuming it to be a technical issue, would call their IT people who changed the setting of the computer workstation prevent timing-out, which would fix the problem for a few weeks, then it would recur again. In determining the root cause of the problem, I reviewed the facility's process and system as a whole and was able to determine that for security reasons, the workstation was configured to receive VA software updates which kept resetting it to time-out after 10 minutes of being idle. Part of the solution was that the workstation needed to be reconfigured by the biomedical engineers and IT team together to designate it as a medical device workstation and prevent it from automatically receiving VA security patches. The clinicians who kept calling the IT people had never contacted biomedical engineers because they kept focusing on the computer workstation problem and never looked at it as a medical device problem. By taking an organizational human factors approach, I was able to bring together all the right people in the same room and solve the problems. Our job is to review the reports and determine how best to prevent the problem from recurring. We look at the facility's processes and systems as a whole to determine where safety measures can be implemented to prevent further harm. Sometimes the facility is attempting to address the problem from a single point of view. We take a systems approach by considering the point of view of the end user and others from the organization, such as the biomedical engineer, the clinician, and the support staff. Figure 2 shows the cross pollination of information and problem perception in an effort to raise the varying areas' awareness and understanding of each other's perspectives when addressing issues. For example, we received a report of a medical device on a computer workstation that was timing-out during a procedure that can take up to 120 minutes. The facility, assuming it to be a technical issue, would call their IT people who changed the setting of the computer workstation prevent timing-out, which would fix the problem for a few weeks, then it would recur again. In determining the root cause of the problem, I reviewed the facility's process and system as a whole and was able to determine that for security reasons, the workstation was configured to receive VA software updates which kept resetting it to time-out after 10 minutes of being idle. Part of the solution was that the workstation needed to be reconfigured by the biomedical engineers and IT team together to designate it as a medical device workstation and prevent it from automatically receiving VA security patches. The clinicians who kept calling the IT people had never contacted biomedical engineers because they kept focusing on the computer workstation problem and never looked at it as a medical device problem. By taking an organizational human factors approach, I was able to bring together all the right people in the same room and solve the problems.
- What human factors-based project do you feel made the biggest impact in VHA and why?
- From an informatics perspective, the project having the greatest impact has been the use of TALLman (mixed case) lettering in the area of ordering medications for Computerized Patient Record System (CPRS). Medication names can sound and look the same. When ordering these medications electronically, it is very easy to make an incorrect selection. By displaying the names of medicine using mixed case lettering, you create a human factors visual queue to the user, alerting them that there is another medication that appears similar in name and that they may want to double check the name of the medication being ordered. Last year, I had major role in the deployment of electronic prescribing of controlled substances (EPCS) with CPRS v.29. Initially, the deployment plan was created as an IT centric project, using OIT protocols only for training, education and deployment. However, the end users, physicians and providers would now be ordering medications using a PIV card, which was previously not required to order medications in CPRS. This was a major change in workflow for them. For EPCS to work correctly, Drug Enforcement Administration credentials need to be appropriately linked to their user name and PIV credentials. By approaching the project just from an IT standpoint, the actual end users prescribers and the staff who support those (Clinical Application Coordinators (CACs), pharmacists, credentialing and privileging, PIV sponsors, etc) were completely overlooked. I bridged the organizational gaps and worked with staff across multiple central offices to create a pre-installation guide for local facilities to use. The guide recommended the creation of a local implementation team comprised of not only IT, but also end users and other staff such as CACs and pharmacists and from a human factors standpoint, walk through together what a user would need for this system to work properly. As a result of bringing the human factors elements together in this way, the VA deployment of a new process to order medications to approximately 100,000 prescribers went relatively smooth and was a success story.
- Where do you see the greatest potential for the application of human factors principles in VHA?
- The biggest area for application of human factors principles in VHA, as well as in health care overall, is in the area of purchasing, contracting, and acquisitions. As the largest provider of health care in the country, VA is able to insist that vendors improve product design. There is no reason we should have to accept or work around poorly designed products. For example, NCPS worked with manufacturers and vendors to create specific syringes designed for U500 insulin administration, as opposed to users working around the problem by using other syringes which can lead to incorrect dosing. We have also seen IV pumps with poor interface design and have had those pumps removed from the purchasing contract.
- Have you seen changes in the interest in or awareness of human factors in VA? What are they?
- The interest and awareness of human factors in VA has definitely been expanding. When I came to VA in 2007, it was engaged in a yearlong pilot of the Patient Safety Fellows Program. Prior to that, VA had not created a training program for post-residency trained physicians and post-doctoral or post-masters degree trained associated health professionals (such as nurses, psychologists, pharmacists, social workers, and health care administrators) to receive in-depth patient safety training that included human factors engineering principles. I've seen this training expanded to residency programs and we now have Chief Residents in Quality and Safety. This expansion is laid upon the foundation of all the human factors work and training conducted by the NCPS. NCPS also helped support the creation of the Informatics Patient Safety Office, who has their own human factors branch where they work with software design and usability. NCPS has now teamed up with Healthcare Technology Management, to offer patient safety and human factors training to biomedical engineers and Technical Career Fields (TCF) interns. Patient Safety and Human Factors training from NCPS is offered a couple of times per year and is required for all biomedical engineering TCF interns.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Can Eye Tracking and Electronic Health Record Mouse Activity Tell us when Clinicians are Overloaded?
[1] Alan Calvitti, PhD [2] Nadir Weibel, PhD [3] Harry Hochheiser, PhD [4] Lin Liu, PhD [5] Kai Zheng, PhD [6] Charlene Weir, PhD [7] Shazia Ashfaq, MD, MBA [8] Steven Rick, BS [9] Zia Agha, MD, MS [10] Barbara Gray, MA [11] Colleen Emmenegger, MS
The amount of thought and attention needed to complete complicated tasks – known as “cognitive load” – can have an impact on physicians’ ability to accomplish important tasks with electronic health records (EHRs). To better understand when physicians experience cognitive load, we are conducting an ongoing usability study of VA’s EHR, the Computerized Patient Record System (CPRS). Based at VA San Diego, this study focuses on clinicians’ cognitive load during outpatient visits. We are using usability software and an unobtrusive eye tracking device to record profiles of clinicians’ activity during the visit, including mouse and keyboard activity from CPRS, as well as clinicians’ eye motion patterns when looking at the monitor. In this paper, we describe example visits by three established clinicians (expert users of CPRS) who were also interviewed in “stimulated recall” sessions, during which they were asked to describe their actions as they watched recordings of the visits. Physicians were also asked to complete a self-reported questionnaire that was then used to compare their experiences of cognitive load. This questionnaire reflects visit-level CPRS-related factors including mental and physical demand, time pressure, performance, frustration, and satisfaction with patient interaction. Based on this evidence we discuss hurdles in relating activity profiles to cognitive load, attention, and safety in clinical settings.
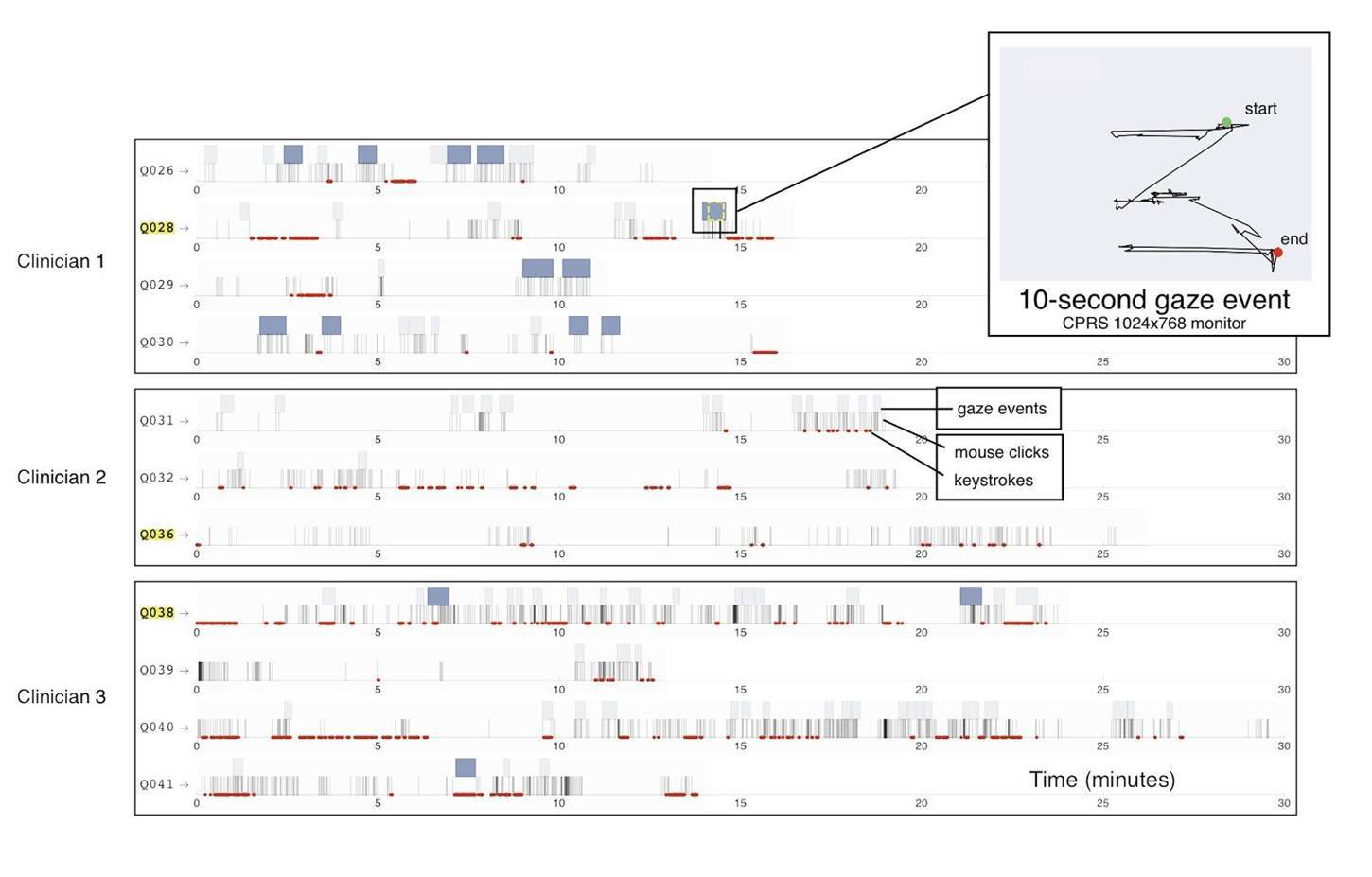
Figure 3 shows the combined mouse and keyboard activity for 11 visits for these three clinicians, along with gaze events representing intervals during which clinicians looked at their CPRS monitor for longer than five seconds. The figure summarizes the large volume of data as chromograms, graphics that display time-stamped mouse, keyboard, and gaze activity along the time axis of the visit. The inset shows a 10-second gaze event displaying “fovea sweep,” where the eyes rapidly scan across a scene to integrate visual detail in the high-durations. Pupil dilation can be extracted and linked to the CPRS content displayed during the corresponding time period. This enables comparison of attentive behavior and observation of errors or discrepancies during EHR tasks (e.g., documentation, information retrieval, order entry) across clinicians, visits, or events of interest.
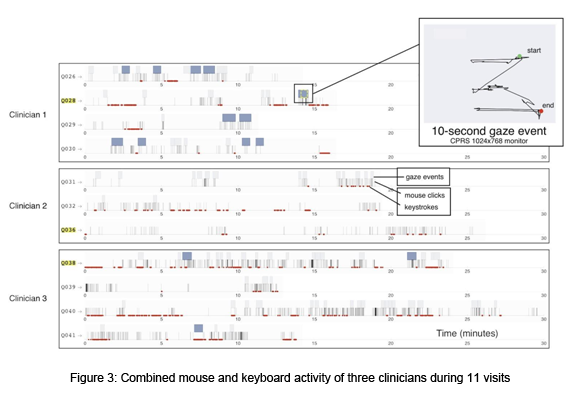
We chose three patient visits to illustrate potential links between time-resolved activity and cognitive load. Overall, all clinicians tended to gaze at the EHR while they were using the mouse rather than the keyboard, as expected. In most visits, clinicians extensively shifted attention between patient interaction and EHR tasks, as well as across various EHR functions. Clinician 1 had 99 mouse clicks, 603 keystrokes, and gazed at the EHR monitor nearly four minutes during a ~16-minute visit. Compared to a larger sample of seven clinicians (37 visits), Clinician 1 scored his/her highlighted visit as moderately to highly mentally and physically demanding, and rated time pressure, effort, frustration, and patient interaction as moderate to high, while scoring self-performance lower. This clinician commented that the information in CPRS is not presented in a patient-centered manner and therefore s/he prefers to share medical data, such as imaging results, by sketching on paper rather than having her/his patients view the data on the monitor. Clinician 2 used the EHR less (155 clicks, 122 keystrokes) than Clinicians 1 and 3; with only 28 seconds of gazing at the monitor during a ~26-minute visit (Q036). Clinician 2 scored his visit as highly demanding both mentally and physically, while low in self-performance and patient interaction. He rated time pressure, effort, and frustration moderate to high. Clinician 3 had the highest amount of EHR activity: 422 clicks (1125 keystrokes) and over 11 minutes of gaze events during a ~24-minute visit (Q038). Clinician 3 scored his visit performance and satisfaction with patient interaction high, but rated the visit low in mental and physical demand, and low in time pressure, effort, and frustration. In the stimulated recall session, this clinician claimed to avoid EHR tasks while the patient is in the room. However, we measured consistently high mouse activity.
Relating time-resolved behavior profiles and cognitive load in real world settings is complicated due to environmental factors, methodological limits, and knowledge gaps in models of cognition. External factors that can complicate analysis include visit-specific factors (e.g., patient complexity, length of patient record, new versus established patient) in addition to broader variables such as work schedule and delays. Pressure from time constraints during clinical practice was indicated in our interviews and may increase cognitive load. System-related technical factors may lead to errors, regardless of the EHR user’s cognitive state (e.g., wrong information retrieved by the software, incorrect test results, and delays in care due to poor communication systems).
Our analysis does not assume that cognitive overloading is the primary cause of safety problems and inefficiency. Relating cognitive load to particular observable adverse outcomes is complicated by multiple factors contributing as causes of errors. For example, diagnostic errors are “intensely personal: the ‘system’ appears to be the physician, and his or her own knowledge, skill, values and behavior.” Cognitive decision processes can be partitioned into the “fast and frugal” System 1 (automatic, effortless, intuitive), and the “slow and deliberate” System 2 (effortful, analytic, algorithmic). System 2 thinking requires concentration and is associated with high cognitive load. This system works well for complex problems, particularly during routine tasks, but is known to fail in novel situations, can be too slow in “decision-dense” environments, and is associated with selective attention blindness. However, System 1 thinking is based on experience and heuristics (i.e., using mental short-cuts and rules of thumb). This effortless processing has low cognitive load but is prone to error through predictable biases: “search-satisficing” (e.g., failing to look at potentially relevant portions of the patient record), confirmation, attribution and framing biases, and many other types. It’s not clear which of these types of thinking is more prevalent and more important for safety. The time pressure of typical clinical workflow suggests that fast thinking, and its attendant cognitive under-loading, should be investigated as carefully as overloading.
Despite these limitations, we believe that a quantitative approach combining activity data in real clinical settings with the context provided by CPRS users’ feedback can help us understand attentive behavior and provide usability metrics to help address safety issues in addition to clinical workflow efficiency.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
Gaining Value from Baseline Business Process Modeling
Brad Branham, Supporting Analyst / Project Lead, Office of Quality, Safety, and Value (QSV), Product Effectiveness; Ferenc Ayer, Program Manager, QSV, Product Effectiveness
Business process modeling (BPM), or workflow mapping, provides an organization with a mechanism to understand its processes through different aspects (such as user roles, technology enablers, or governing statements) and in turn, activities from which the organization derives value. The development of a business process model is a fundamental starting point as it provides the “context” within which all process management and improvement is carried out. BPM can have a significant impact on human factors by enabling insights into users’ workflow requirements independent of current technology enablers. Furthermore, human factors can impact business process design and the resulting effectiveness and value.
We conducted an analysis of as-is processes specific to pre-defined  organizational domains (e.g., clinical service) or as an integrated workflow (e.g., inpatient flow through a polytrauma episode of care) to help define value derived from current processes, identify pain points that are reducing value (problem space), and to estimate return on investment (ROI) from process improvements. The process model enables an organization to make a clear link between the performance improvements they are trying to achieve and the processes which contribute to that performance. Some of the human performance indicators that the BPM can help understand are: organizational domains (e.g., clinical service) or as an integrated workflow (e.g., inpatient flow through a polytrauma episode of care) to help define value derived from current processes, identify pain points that are reducing value (problem space), and to estimate return on investment (ROI) from process improvements. The process model enables an organization to make a clear link between the performance improvements they are trying to achieve and the processes which contribute to that performance. Some of the human performance indicators that the BPM can help understand are:
- Greater clarity about the purpose or value of each step within a process (such as a medication order) and its contribution to organizational goals, which provides evidence to support a business case for a new investment and its requirements
- Clear definition of boundaries and dependencies between key processes, which may expose workarounds and bottlenecks in the process
- Time cost of process and frequency of process use
- Information (and other resource) needs and artifact use
- An understanding of the need for process owners/managers and their role in driving performance improvement
- A clear set of priorities and targets for process management, such as Key Performance Indicators (KPIs) linked to strategic goals
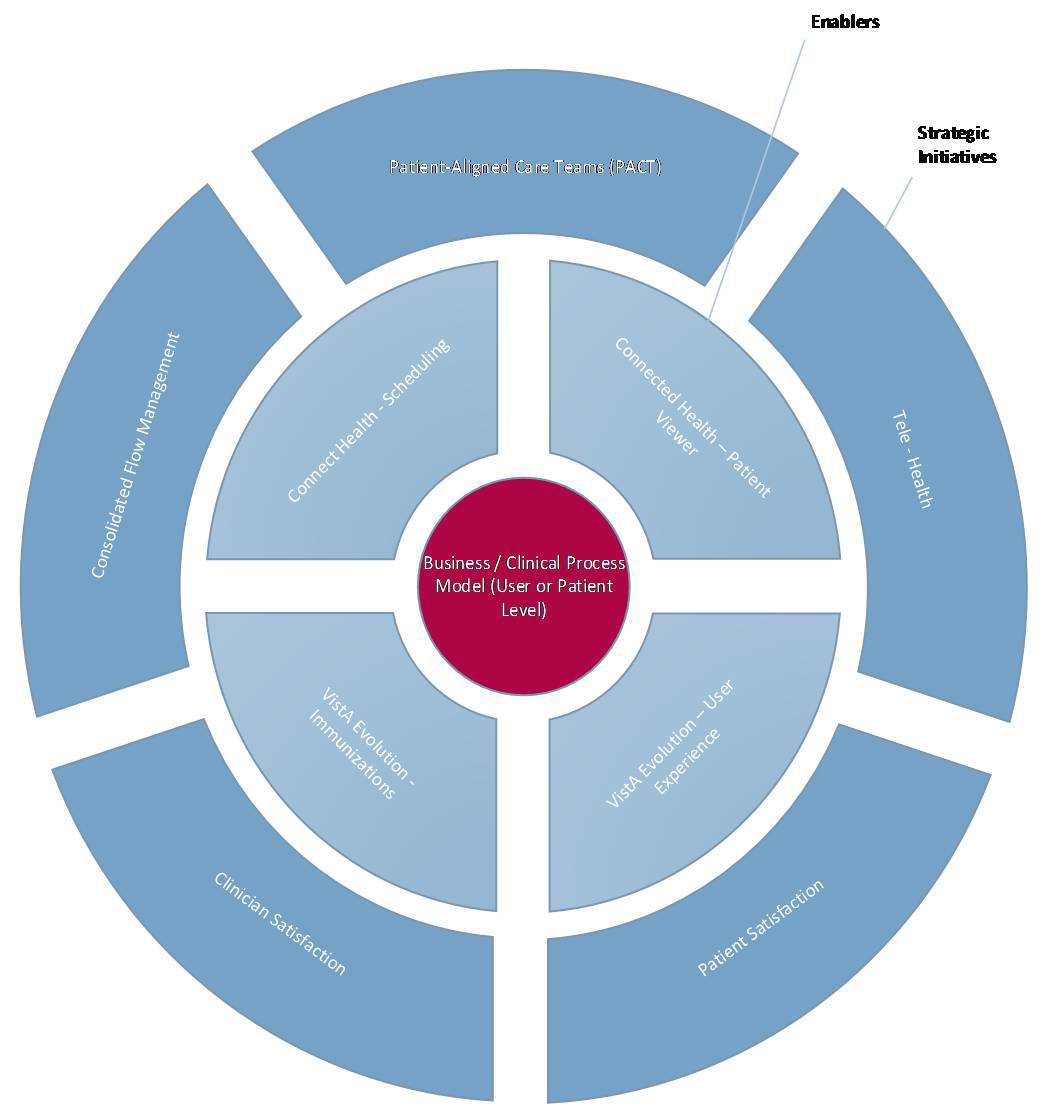
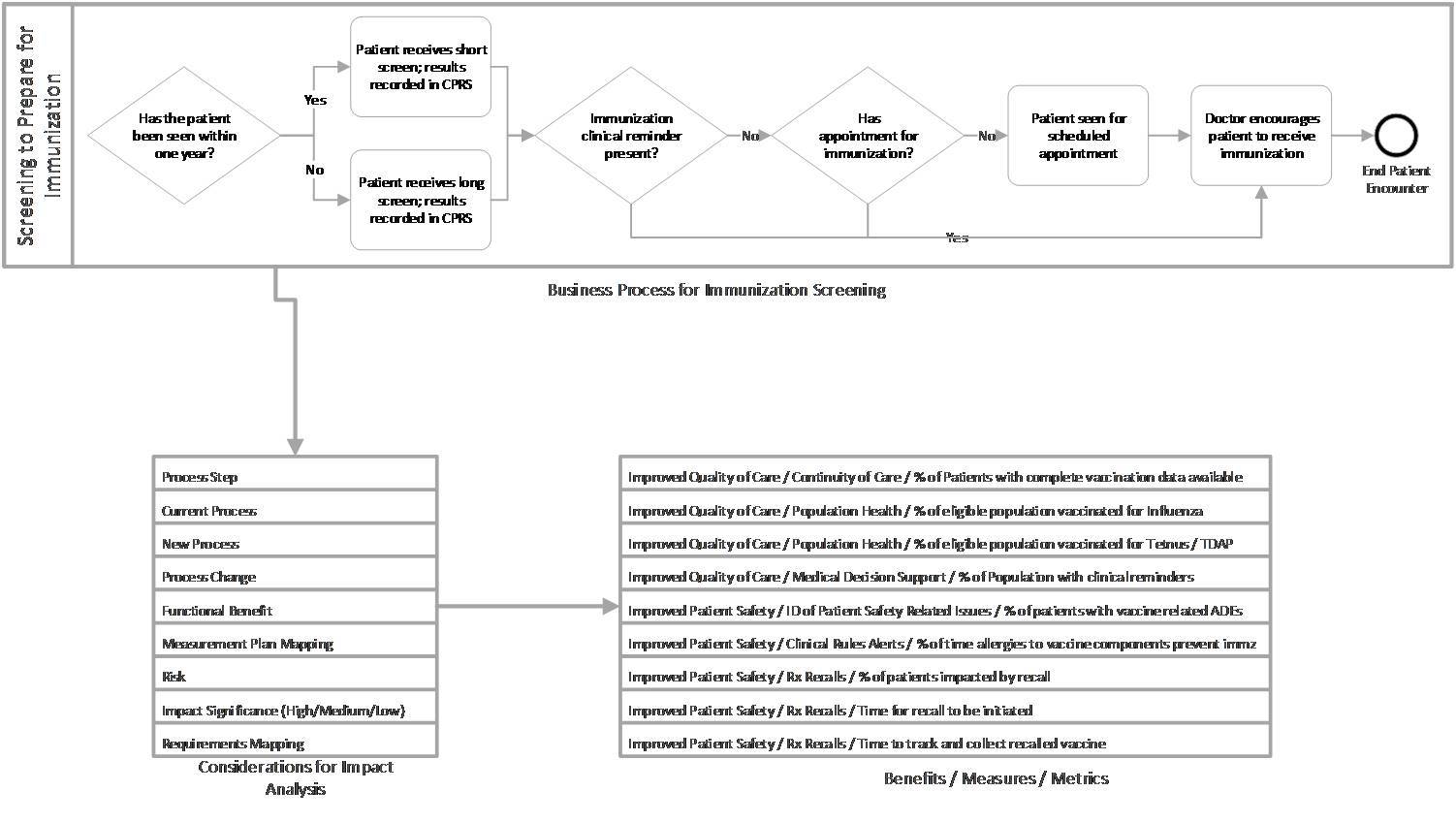
Without understanding what a process model brings, an organization risks investing in a series of tactical improvement projects without seeing the big picture and without making the connections across the processes that add the most value. The BPM in Figure 5 enables a comparison of current functionality/process to future functionality/process in order to provide insight into potential impacts, and offers an assessment of benefits to be realized from the investment.
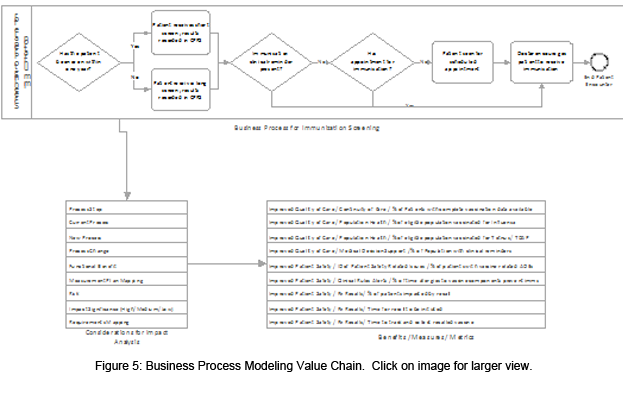
The comparison of current state to future state functionality and workflow helps to identify the following key components to assessing the impact of introducing change into a current process:
- Potential Process Change – the current process documented in the baseline BPM compared to the potential future process once the change is deployed, supporting systems design
- Functional/Business/Clinical Benefits – the utility provided by the change which is expected to provide a benefit to the user/organization, to be captured in Product Effectiveness’ Measurement Plan
- Potential Risks – risks to achieving potential benefits based on knowledge of the current processes and expected impact of change
- Potential Significance of the Impact – the order of magnitude in which the new tool may impact the current process, which may set acceptable target values for performance measures
Identifying these key areas as part of an impact analysis helps to pinpoint potential areas of benefits and measures that can be incorporated into the measurement plan to guide the execution of baseline and post measurements, thus reflecting the value and effectiveness of the investment. Figure 5 shows BPM as a dependency to create a cohesive, coherent workflow understanding between organizational initiatives and supporting programs (such as VistA Evolution and Connected Health) and how Health Information Technology (HIT) can support design decisions for Patient Aligned Care Teams, telehealth, etc. BPM is an increasingly important collaboration tool for helping to facilitate communications, reduce redundancy, and clarify overall value.
While business process models have been used to aid in the development of key performance indicators and respective measurement plans to assess the effectiveness and value of an investment, there are opportunities to optimize the value of a BPM effort across organizations and programs, such as:
- Identifying all governing statements (policies, standards, guidelines etc.) for each process improvement to assess what is driving the behavior of a process component
- Leveraging insights into the integration of people, processes, and technology capabilities to drive system designs, process re-engineering efforts (including human factors engineering), and definition of usability measures
- Identifying all decision points within a process flow which could support an alternatives analysis
Within an integrated healthcare environment, such as VHA, enterprise-wide problems need to be solved, and every process change can have an unintended cascading effect within the health system. Introducing business process modeling efforts within the organization begins to identify holistic problems to be solved, enabling correlations of workflows and initiating the planning phases to effectively solve enterprise-wide change.
A common pitfall with workflow modeling is that the models often do not separate the work that needs to be done from the specific technology currently used to complete the work. An existing workflow may be linked to technology that is currently in use to support the work. However, if new technology is being conceived to enhance the work processes, it is important to understand the constraints of the work independent of the current HIT solutions in place. Business process modeling ensures the work processes are represented at a level of abstraction that is independent of the current technology used to support the work, so that the impact of introducing new technology on the work processes can be clearly understood. As such, workflow modeling can provide a needed foundational understanding of a process to support human-technology integration considerations for both existing and new HIT tools.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|

 Mobile Application Design Brief: Cognitive Load Mobile Application Design Brief: Cognitive Load
Donna Harrigan, BA, Management and Program Analyst, HFE, Health Informatics Division, Office of Informatics and Analytics
In previous issues of this newsletter, I’ve written about user interface (UI) design standards and best practices such as the use of simplicity and minimal design to highlight key information on a page and consistency in navigation and terminology to provide familiarity for a user. The common goal is to make it easier for a user to get the information 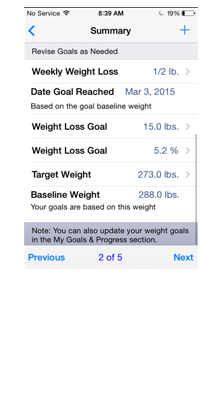 needed to perform a task or make a decision. An app should be designed so the user can effortlessly comprehend the information presented, while staying focused on the task or decision at hand. needed to perform a task or make a decision. An app should be designed so the user can effortlessly comprehend the information presented, while staying focused on the task or decision at hand.
There are techniques a developer can use to minimize the user’s cognitive load, such as effectively grouping information on a page (avoiding multiple pages) and keeping all selection choices visible at the same time (circumventing scrolling). Kathryn Whitenton from the Nielsen Norman Group recommends: “Look for anything in your design that requires users to read text, remember information, or make a decision. Then look for alternatives: can you show a picture, re-display previously entered information, or set a smart default?”
The screen image shown in Figure 6 is taken from VA/VHA developed “MOVE! Coach Mobile” app and does a great job of helping user cognition in this manner. Each week the user completes a set of guides, and at the end of each guide, a reminder screen of goals is displayed. Changes are allowed at this point rather than requiring the user to go through the “My Goals and Progress” section. This direct access to information lessens the cognitive load on a user by eliminating the need to remember to update goals, and also from having to remember the navigation steps to perform the updates.
|
Back to top of article | Back to article summary | Back to top of newsletter
|
|
|
 |
|