|
Back to TOP

Goa and Telangana Regulators Eligible to Observe FDA Inspections Following First Joint FDA Forums
After participating in joint regulatory forums organized by the FDA’s India Office (INO), drug regulators in two of India’s 29 states – Goa and Telangana – have joined the group of eligible states to observe inspections conducted by the FDA in India.
The first Annual Regulatory Forum with Goa’s Directorate of Food and Drugs Administration (DFDA) was held October 18-19, 2023, while the first Annual Regulatory Forum with the Telangana Drugs Control Administration occurred on January 31, 2024.
Both inaugural forums were designed to share inspectional best practices for medical products and served as an opportunity for the FDA and state regulators to provide an overview of regulatory operations and learn about one another’s current compliance practices to better inform future engagements.
 FDA India Office and Telangana Drugs Control Administration participants at the forum in Telangana.
Medical product topics covered by INO staff at the meetings included the history of the FDA’s drug regulations, the basic elements of a robust Pharmaceutical Quality System, and the value of a risk-based approach to Good Manufacturing Practice inspections. FDA staff then discussed the elements of the agency’s Observed Inspection standard operating procedure — this process allows Indian inspectors to be invited to observe select FDA medical product inspections, one of the activities to be planned and performed under a Memorandum of Understanding that the FDA signed with India in 2020. By participating, Indian regulators can improve their capacity for regulatory oversite of medical products.
In India, laws regulating medical products are established at the national level but enforced by both central and state governments. One of INO’s important goals at these forums was providing detailed information on FDA inspectional practices so that state regulators could qualify to participate as observers of FDA inspections along with India’s national regulatory counterpart, the Central Drugs Standard Control Organisation (CDSCO).
 Presenters from the FDA's India Office at the forum in Telangana (left to right, top row then bottom): Dr. Sarah McMullen, Dr. Phil Nguyen, Yvins Dezan, Dr. Sudheendra Kulkarni, Guerlain Ulysse, and Karthik Siva Chaitanya.
Once a state achieves that status, the FDA notifies the CDSCO. Goa and Telangana have now become the third and fourth states, respectively, to reach this milestone, along with Gujarat and Karnataka.
Often referred as the “Bulk Drug Capital of India” and “Vaccine Capital of the World,” Telangana accounts for:
- Over 40% of the total Indian active pharmaceutical ingredients (API) production.
- More than 35% of total pharmaceutical production in India.
- Approximately 50% of API exports from India.
- One-third of global vaccine output.
Goa, located on the coast of the Arabian Sea, is India’s smallest state by area but an established base for the pharmaceutical industry and an emerging destination for the biotechnology and IT industries.
 FDA India Office and Goa DFDA participants on the second day of the forum in Goa.
The first day of the multiday Goa forum was devoted to food regulation. It featured a presentation on food facility inspections from the perspective of an FDA investigator. INO consumer safety officers also reviewed the FDA’s food safety regulations and facilitated a group discussion using a seafood inspection scenario. Among the other topics of discussion were INO’s role in enhancing the safety of food imported into the United States, Goa DFDA and India’s food regulations, and Indian programs for regulating and inspecting food products intended for export. The state is known for its seafood, spices, and jackfruit, and continues to grow its infrastructure for exporting its goods globally.
 Presenters from the FDA's India Office at the forum in Goa (left to right, top row then bottom): Dipesh Shah, Dhruv Shah, Greg Smith, Kelia Hicks, Jake Lane, Kunapuli Madhusudhan, and Dr. Pankaja Panda.
INO's Good Clinical Practice Training Draws Crowd
It was standing room only at the Indian Society for Clinical Research Pre-Conference in Hyderabad on February 1 for a daylong training offered by the FDA’s India Office (INO) on an important aspect of the drug business – the conduct of clinical trials.
Specific to generic drugs and particularly relevant in India, companies must submit study data to the FDA demonstrating that their drug is therapeutically equivalent to the branded drug and show that human subject studies conducted to support approval must comply with good clinical practices (GCPs) requirements as part of the application process. These requirements are intended to ensure data quality and integrity and to protect the rights and welfare of the human subjects.
To ensure GCP compliance, the FDA inspects clinical sites — what the agency calls bioresearch monitoring, or "BIMO." India is an important source of generic drugs — nine out of 10 drugs prescribed in the U.S. are generics, and 40% of those drugs come from India — so it’s not surprising that many of these BIMO inspections are conducted in India. In fact, nearly 33% of the FDA’s foreign clinical trial inspections occur in that country.
During INO’s interactive presentation, generic drug sponsors and contract research organizations listened to case studies and investigator observations and discussed GCP best practices. It was INO’s sixth and perhaps most productive engagement, with 100 participants, double the number of participants from past years.
“It was gratifying to see such active engagement at this year’s conference,” said INO Director Sarah McMullen. “It reflects, I think, an increasing desire to understand the practicalities of current GCPs globally and their implementation.”
In addition to the FDA’s appearance at the pre-conference, McMullen delivered a keynote address on patient centricity in clinical trials at the main conference where the topic this year was "research transformation to better patient outcomes."

FDA Publishes Revised Draft Guidance on Remote Regulatory Assessments
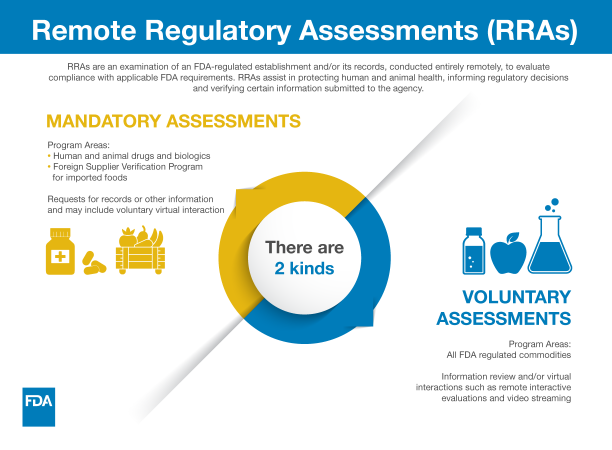
The Food and Drug Administration recently published a revised draft guidance for industry titled Conducting Remote Regulatory Assessments Questions and Answers. A Remote Regulatory Assessment (RRA) is an examination of an FDA-regulated establishment and/or its records, conducted entirely remotely, to evaluate compliance with applicable FDA requirements.
Some of the tools used in RRAs include remote records requests, remote livestreaming video of operations, teleconferences, and screen-sharing. These approaches have enabled the agency to provide oversight to as many facilities as possible when travel was restricted while continuing to deploy resources where possible to protect consumers and patients and promote public health.
Throughout the pandemic, for example, the FDA used RRAs both domestically and abroad for certain FDA-regulated products to help the agency conduct oversight, mitigate risk, and meet critical public health needs when inspections could not be conducted. For example, RRAs assisted the FDA in verifying corrective actions taken in response to inspections of previously compliant manufacturers. They have provided information about deficient practices, leading the agency to take regulatory actions and/or conduct inspections, while informing future inspection planning. RRAs also were used to help support review and promote timely approval or authorization of marketing submissions for FDA-regulated products. In the FDA’s food program, RRAs have helped to determine compliance with veterinary feed directive regulations, assess foreign manufacturing process records, add foreign establishments to import alerts, and issue warning letters.
 Because of the effectiveness of these tools, the agency will continue to use RRAs when appropriate in overseeing industry and ensuring the safety and effectiveness of all types of regulated products, supplementing critical oversight tools such as inspections.
The draft guidance, once finalized, will describe how the FDA will use RRAs for FDA-regulated products. The revised draft guidance reflects the agency's consideration of comments to draft guidance from July 2022, as well as revisions to align with recent changes in law concerning mandatory records requests. The FDA welcomes public comments on the draft guidance during the 60-day comment period via the Federal Register website.
FDA Co-Hosts Workshop in Peru on Whole Genome Sequencing
 The FDA’s Office of Regulatory Science in the Center for Food Safety and Applied Nutrition (CFSAN) and the United Nation’s Food and Agriculture Organization hosted a joint workshop in Lima, Peru, in late January on how whole genome sequencing (WGS) can be used to prevent and respond to water- and foodborne outbreaks. In addition to experts in Peru, the workshop drew members of the Latin American Surface Water Surveillance Program, which CFSAN supports through a cooperative agreement with the Maryland- based Joint Institute for Food Safety and Applied Nutrition. In that program, participants isolate and sequence Salmonella enterica from South American surface waters associated with crop irrigation, including rivers, reservoirs, irrigation channels, ponds, lakes, streams, creeks, and irrigation canals.
The workshop focused on summarizing the state of the current technology, various sequencing networks, and how data can be shared within and between interoperable networks. Peru participates in the GenomeTrakr network, a network of public health and university laboratories that collect and share genomic and geographic data regarding foodborne pathogens. The data (over 1.2 million samples) is housed in public databases at the National Center for Biotechnology Information and can be accessed by researchers and public health officials for real-time comparison and analysis that can speed foodborne illness outbreak investigations and reduce foodborne illnesses and deaths. To date, Peru has uploaded over 5,000 sequences into this international database.
At the workshop, experts also exchanged ideas on the proposed solutions —and related challenges — for transitioning to a more robust whole genome sequencing food safety program in Peru, which would require greater resources and sectoral coordination.
FDA subject matter experts Dr. Marc Allard and Dr. Narjol Gonzalez-Escalona were speakers and the Latin America Office's point of contact for WGS, Bruce Ross, also joined for liaison and in-person interactions with seminar participants.
CVM Develops Draft Guidance on GMPs for Veterinary Active Pharmaceutical Ingredients
 On January 24, the FDA’s Center for Veterinary Medicine announced the availability of a draft guidance for industry (GFI) #286 (VICH GL60) entitled, “Good Manufacturing Practice for Active Pharmaceutical Ingredients used in Veterinary Medicinal Products.” This draft guidance has been developed by the International Cooperation on Harmonization of Technical Requirements for Registration of Veterinary Medicinal Products (VICH).
VICH is a trilateral program officially launched in April 1996. The program aims to harmonize technical requirements for the approval of veterinary medicinal products in the European Union (EU), Japan, and the United States, and includes input from both regulatory and industry representatives. In support of wider international harmonization of regulatory requirements, VICH guidelines are also available for use by other countries.
This draft guideline has been developed based on a similar guideline (ICH Q7: Good Manufacturing Practice for Active Pharmaceutical Ingredients) intended to cover human drugs from the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH). The objective of this draft guidance is to provide recommendations regarding good manufacturing practices (GMPs) for the manufacturing of active pharmaceutical ingredients (APIs) for use in veterinary medicinal products. It facilitates harmonization of a single set of international standards for GMP inspections of facilities that manufacture APIs and starting materials for use in such products. It also allows manufacturers and regulators a framework to ensure that APIs meet the quality and purity characteristics that they are intended to possess.
The FDA’s work with VICH aims to ensure regulatory certainty for veterinary products, including predictable and uniform requirements across the EU, Japan, and the United States. The collective work also helps to reduce animal testing, facilitate trade, and ensure veterinary product safety and consumer confidence in the regulated products.
To submit comments electronically, visit Regulations.gov and type the following docket number into the search box: FDA-2023-D-4761. The agency requests submissions be made by March 25, 2024, to ensure that the FDA considers your comment(s) before it begins work on the final version of the guidance document.
FDA to Host International Medical Device Regulators Forum
The U.S. Food and Drug Administration (FDA), as the Chair and Secretariat of the International Medical Device Regulators Forum (IMDRF), will host the 25th Session of the IMDRF in Washington, D.C., on March 11-15, 2024.
The first two days of the meeting are free and open to the public and will be offered either virtually or in person. Day One is a joint IMDRF-Industry workshop on the topic of medical device regulatory reliance, exploring such topics as what reliance is and why it is important, reliance in a premarket setting, and reliance in a postmarket setting. Day Two will feature regulatory updates from the IMDRF Management Committee and IMDRF’s Official Observers. The last three days, March 13-15, are for IMDRF invitees only.
 In September, the FDA’s Center for Devices and Radiological Health issued a draft International Harmonization Strategic Plan to encourage harmonization, convergence, and reliance among medical device regulatory authorities. That plan defined reliance as an act whereby the regulatory authority in one jurisdiction may take into account and give significant weight to assessments performed by another regulatory authority or trusted institution, or to any other authoritative information in reaching its own decision. The relying authority remains independent, responsible, and accountable regarding the decisions made, even when it relies on the decisions and information of others.
The IMDRF forum will be held at the Ronald Reagan Building and International Trade Center located at 1300 Pennsylvania Avenue NW in Washington, D.C. Space is limited for in-person attendance and early registration is encouraged. The public can also attend the meeting via livestream. Registration for in-person attendance closes on February 16, 2024.
The IMDRF was established in October 2011 and is a voluntary forum for medical device regulators from different jurisdictions who have agreed to work together to advance international regulatory harmonization and convergence in the field of medical devices.
The forum develops internationally agreed-upon documents related to a wide variety of topics affecting medical devices. When finalized, IMDRF members adopt these documents where appropriate, and in some cases adapt them to meet the regulatory requirements of their jurisdictions.
The IMDRF Management Committee includes representatives from Australia, Brazil, Canada, China, the European Union, Japan, Russia, Singapore, South Korea, the United Kingdom, and the United States. Argentina, Switzerland, and the World Health Organization are official observers to the IMDRF. Affiliate Members are Chile, Cuba, Egypt, Israel, Montenegro, South Africa, and the Taiwan Food and Drug Administration.
FDA and EMA Host Discussion Panel on Significant Advances in Cancer Treatments and Therapies
The FDA’s Oncology Center of Excellence (OCE) recently collaborated with the European Medicines Agency (EMA) in hosting “Conversations on Cancer: Transforming Patient Lives by Therapeutic and Regulatory Innovations,” on February 1.
The panel discussion, which took place ahead of World Cancer Day on February 4, focused on three forms of cancer – multiple myeloma, chronic myelogenous leukemia (CML), and melanoma – all of which have experienced significant advances over a 25-year period. The panelists were asked why progress was made in these diseases and what was the role of regulatory agencies, scientists, and clinicians in achieving this progress.
 “When I take a look at these diseases, I’m amazed at the progress that’s been made,” said OCE Oncology Director Richard Pazdur, M.D. “I’ve covered a wide variety of patients throughout my clinical career within these three diseases. You still see the faces and ask yourself, what would be their stories be now. It’s a tragic irony that treatments used today were not available then.”
Both the FDA and EMA have programs in place to expedite the development and review of new drugs to address unmet medical needs in the treatment of serious or life-threatening conditions.
The FDA’s accelerated approval program, initially developed for HIV/AIDs drugs in the 1990s, is a popular path to market for oncology drugs. Under this program, products are approved based on a surrogate endpoint that is thought to predict clinical benefit but is not itself a measure of clinical benefit. The use of a surrogate endpoint can considerably shorten the time required prior to receiving FDA approval. In oncology the surrogate endpoint may be tumor shrinkage or a composite endpoint where an event is defined as either growth of tumor beyond an arbitrary threshold (progression) or detectable recurrence of disease, or death. Drug companies are still required to conduct studies to confirm the anticipated clinical benefit. If the confirmatory trial shows that the drug actually provides a clinical benefit, then the FDA grants traditional approval for the drug.
Currently over 75% of the products approved for marketing under the accelerated approval program are for treatment of malignancies, said Pazdur. Over time, the accelerated approval program has evolved to single-arm trials for oncology products where all patients with the targeted medical condition are given the experimental therapy and then followed over time to observe their response. This is in contrast to a randomized trial where patients are randomly selected to receive one of two or more therapies and then compared.
The EMA has its own accelerated approval program, a priority medicines scheme that it calls PRIME. This voluntary scheme targets unmet medical needs and is based on enhanced interaction and early dialogue with developers of promising medicines, to optimize development plans and speed up evaluation so these medicines can reach patients earlier.
In addition, the EMA has another program that supports the development of medicines that address unmet medical needs – conditional marketing authorization. Applicants may be granted a conditional marketing authorization for such medicines on less comprehensive clinical data than normally required, where the benefit of immediate availability of the medicine outweighs the risk inherent in the fact that additional data are still required. Conditional marketing authorizations are valid for one year and can be renewed annually. Once a conditional marketing authorization has been granted, the marketing authorization holder must fulfill specific obligations within defined timelines. These obligations could include completing ongoing or new studies or collecting additional data to confirm the medicine's benefit-risk balance remains positive. An estimated 80-85% of approvals under conditional approvals are oncology drugs, including several drugs used to treat multiple myeloma.
Patient advocates — Jan Geissler from Germany, Fredrik Ostman from Sweden, and Yelak Biru from the United States, were three of the nine panelists. Geissler, a CML patient since 2001, benefited from imatinib — a drug that has revolutionized CML treatment today – when it was an experimental treatment. Ostman was diagnosed with melanoma in 2014 — and currently has no evidence of the disease. Yelak Biru’s was diagnosed with myeloma in 1995 and has been in remission for decades.
“Since 2003, there are almost 20 approved drugs to treat multiple myeloma. Life expectancy has changed from two to three years to 10 or more for standard risk patients, but challenges in getting treatments to patients early on, remains a challenge,” Biru said.
This event was the second collaboration between the FDA and EMA. Previously, the two agencies hosted a discussion with breast cancer patients diagnosed with advanced-stage or metastatic disease in October.
The Oncology Center of Excellence’s Conversations on Cancer series started years ago as an internal program to educate FDA staff outside of OCE on oncology advancements and treatments. OCE leadership expanded the series – with the help of technology – to an external, worldwide audience.
The event was hosted on YouTube and recorded with subtitles. Attendees were able to post comments and questions to OCE’s X account (formerly known as Twitter).
FDA Partners with ROK for AI Regulatory and International Symposium in Seoul
The FDA and the Republic of Korea’s Ministry of Food and Drug Safety (MFDS) are co-hosting a joint symposium from February 26-29 in Seoul on the use of artificial intelligence (AI) in the medical products industries.
 The Artificial Intelligence Regulatory and International Symposium (AIRIS) 2024 is the realization of a Memorandum of Cooperation (MOC) between the FDA and the MFDS to facilitate a joint workshop on the topic. FDA Commissioner Robert Califf, M.D., and MFDS Minister Yu-Kyoung Oh signed the MOC April 27, 2023, in Washington, D.C. Moreover, “exchanging information about the safe production of medical products with AI” was one of the further cooperative activities cited in a White House Fact Sheet following a state visit by Republic of Korea President Yoon Suk Yeol to Washington that same week.
This month’s symposium will feature speakers from global government agencies, industry, and academia, and focus on the use of AI in a wide range of medical products including biologics, pharmaceuticals, and medical devices. Seven sessions are planned and will cover such topics as transparency, explainability, and bias; technology trends (including machine learning for clinical decision support systems and using AI for safety surveillance); and what direction regulators should go in cooperating on the regulatory aspects of AI to ensure that medical products that use this technology remain safe and effective.
OGPS Senior International Policy Advisor Sema Hashemi will represent the FDA at the symposium along with Hussein Ezzeldin, Digital Health Technology Review Team Lead, Center for Biologics Evaluation and Research. The FDA delegation will also include the Center for Drug Evaluation and Research’s Tala Fakhouri, Associate Director for Policy Analysis; Mira Jacobs, Acting Assistant Director for the Digital Health Policy Team; Anindita Saha, Assistant Director for Partnerships and Regulatory Science; and Melissa Torres, Associate Director for International Affairs, Center for Devices and Radiological Health.
For more information, visit AIRIS 2024.
|