|
 
September 2023
Volume 23, Issue 9
The U.S. Food and Drug Administration’s (FDA) MedSun program provides this monthly newsletter to inform patients and patient advocates about FDA-related information on a variety of topics, including new products the FDA has authorized for marketing, significant labeling changes, safety warnings, notices of upcoming public meetings, proposed regulatory guidances and opportunity to comment, and other information of interest to patients and patient advocates.
The MedSun program, launched in 2002 by the FDA’s Center for Devices and Radiological Health (CDRH), involves the reporting of problems with medical products from a network of approximately 300 hospitals, nursing homes, and home health facilities around the United States. MedSun sites work collaboratively with the FDA to assist in detecting, understanding, and sharing information concerning the safety of medical products. MedSun uses a secure, online reporting system for reporting problems with the use of medical devices and plays a critical role in the FDA’s postmarket surveillance efforts..
|
|
Tips for Submitting Comments on CDRH Guidance Documents
Public comments on the FDA's Center for Devices and Radiological Health (CDRH) guidance documents are critical to the guidance development process and help us ensure our recommendations meet stakeholder needs. CDRH has published tips, recommendations, and instructions on how to submit comments for a guidance document on our website.
|
|
|
The reports that follow represent a cross section of device related events sent by MedSun Representatives during the prior month. The reports are presented as submitted by MedSun Representatives and in some instances, have been summarized and/or edited for clarity.
|
|
Type: Ventilator, Continuous, Facility Use
Manufacturer: Draegerwerk AG Co. | Brand: IACS Workstation Critical Care
Model #: 8416400 (35 devices)
Event Description: This user facility is experiencing ongoing issues with the leak compensation feature in the Draeger V500 ventilator. Due to staff concerns that arose while performing patient leak tests, the number of potential false leak results, and a recent patient requiring management of a bronchopleural fistula, the user facility has turned off the leak compensation feature. Following Draeger's instructions for use resulted in a persistent 9-10% leak from the ventilator which was not caught in the breathing circuit system test. In a meeting with Draeger, it was noted that the user facility did not test the V500 with the heater turned on.
Type: Electrosurgical, Cutting & Coagulation & Accessories
Manufacturer: Covidien LP | Brand: ValleyLab | Lot #: 025564
Event Description: The loop on the cautery holster in the breast pack breaks off. The loop is used to secure the holster to the sterile drape and without it, the cautery pencil does not have a protected holding place on the surgical field. This creates the potential for inadvertent pencil activation and increases the risk of a burn or surgical fire. The cautery pencil also can inadvertently puncture the sterile drape. The staff in Breast Service Line report 50% of the holsters fall apart. Staff report "this problem also is occurring in many other manufacturer packs.” The OR Team also reported the surgical pencils used as a single use item do not have the same issues as the ones in the packs.

Type: Pump, infusion, elastomeric
Manufacturer: Avanos Medical, Inc.
Brand: Avanos Homepump C-Series, 270 ml, 5 ml/hr
Model #: 13568
Lot #: 30225018
Cat #: c270050
Event Description: The patient returned to the chemotherapy clinic to have the Avanos Homepump C-Series elastomeric pump disconnected (ambulatory chemotherapy pump). It contained fluorouracil. As the nurse removed the tape securing the sensor, white powder was found under the tape around the sensor indicating a possible drug leak. The patient did not notice damp sensations or leaking from the tubing or pump. The area was cleaned, and the patient stated they did not feel any irritation, itching or discomfort at the site. The patient was instructed to notify the health care provider of any skin changes to that area.
|
Devices 1-4:
Type: Injector and Syringe, Angiographic
Manufacturer: ACIST Medical Systems, Inc.
Brand: ACIST CVi Contrast Delivery System
Brand: A2000 Multi-use Syringe Kit | Cat #: 014612
Brand: AngioTouch Kit | Model #: 014645 | Cat #: 014645
Brand: Bt2000 Automated Manifold Kit | Model #: 014613 | Cat #: 014613
Device 5:
Type: Catheter, Intravascular, Diagnostic
Manufacturer: Terumo Medical Corporation | Brand: Optitorque
Model #: 40-5013 | Cat #: RH5TIG111A
Event Description: The patient was scheduled to undergo a cardiac catheterization to treat possible coronary artery disease. After all appropriate procedures were done to prepare the contrast injection device, the physician injected dye into the coronary arteries through a right radial catheter. The team member monitoring the procedure and recording fluoroscopy noted what looked like air in the left anterior descending artery (LAD) and circumflex arteries with what appeared to be cardiac standstill. Staff immediately alerted the physician and other team members, and emergency measures began. The patient was intubated, and cardiac medications were given. The physician placed a second line and proceeded to perform a percutaneous transluminal coronary angioplasty (PTCA) in the 100% occluded arteries. This was successful with reducing the blockage to 0%. An intra-aortic balloon pump (IAPB) was also placed to assist with cardiac function. However, the medical team was not able to get cardiac function to return on its own. Biomedical’s investigation did not identify issues with the ACIST CVi injector device. However, we could not rule out issues with the other parts of the system including the tubing, syringe, or manifold.
Type: Marker, Radiographic, Implantable
Manufacturer: Merit Medical Systems, Inc. | Brand: Scout
Lot #: H2586282 (x2) | Cat #: SSR75S-01
Event Description:A biopsy of the right breast under ultrasound guidance was performed. The physician attempted to place an imaging marker but did not deploy. Mammography imaging performed as protocol to confirm marker placement. They physician was unable to visualize a marker on mammography. Repeated marker placement was attempted. Mammography confirmation obtained again, and marker was not visualized. Staff confirmed the marker was stuck in the sterile marker packaging. The physician did not realize the markers didn’t deploy until after 2nd mammography image was obtained. The patient refused to allow another attempt to place a marker and left the imaging department. We reached out to the sales representative about the device problem. The sales representative let us know there have been several complaints of the marker being stuck in packaging.
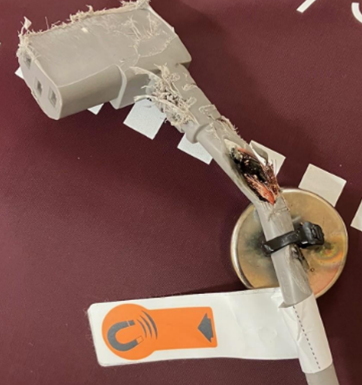
Type: Bed, flotation therapy, powered
Manufacturer: Hill-Rom, Inc.
Brand: Compella Bariatric Bed
Model #: P7800 | Other #: P7803A02
Event Description: The Hill-Rom Compella Bariatric Bed has a power cord which is attached to a blower. The power cord for the blower has a magnet attached which allows the cord to stay secured to the bedframe. Due to the width and length of the bed, the blower was removed from the bed for transporting the bed in the elevator. Staff was unaware of the function of the magnet. Therefore, the power cord was left loose which became entangled in the bed wheels causing fraying of the cord. During patient care, the staff witnessed sparking from beneath the bed. The source was determined to be the power cord to the blower. No patient or staff were harmed during this event. The manufacturer recommended shortening the width and length of the bed instead of removing the blower when transporting.
|
|
|
Neonatal and Pediatric Reports |
|
 |
|
These reports describe medical device events involving neonatal or pediatric patients, or those events involving a medical device that is indicated for use in neonatal and pediatric patient populations.
FDA defines pediatric patients as those who are 21 years of age or younger (that is, from birth through the twenty-first year of life, up to but not including the twenty-second birthday) at the time of the diagnosis or treatment.
|
Type: Infant heel warmer (chemical heat pack)
Manufacturer: Cardinal Health 200, LLC | Brand: Novaplus
Model #: V11460-010 | Lot #: V3A159F | Cat #: V11460-010
Event Description:The phlebotomy technician attempted to activate a heel warmer to use on a patient with difficult venous access. The technician squeezed the pack to activate it and the pack burst, leaking all over the patient's bed. The technician states the patient was not injured and cleaned the contents off the bed. The infant was not affected by the leaked product. NOTE: There was a recall on this product June 16, 2023, but the recalled lot number was different (V2S506).
Type: Clamp, Circumcision
Manufacturer: Centurion Medical Products Corp. | Brand: Centurion
Model #: 330CR6
Event Description: The infant was undergoing circumcision by the OB (obstetrician) doctor who used 1.3 disposable Gomco. Post-circumcision, the infant continued to bleed. The doctor thinks it could be related to a possible defect of the Gomco. The device was saved for evaluation. Post-operative bleeding occurred at 1100 and ended at 1320. During that time, pressure was applied in addition to silver nitrate, and a cold compress. Urology consulted, assessed infant, and placed stitches.
|
|
FDA Meetings, Conferences and Workshops |
|
Links to FDA CDRH Databases and Other Information Sources |
|
U.S. Food and Drug Administration
10903 New Hampshire Ave.
Silver Spring, MD 20993 |
|
|
|
|
