Medicaid Enterprise Certification Toolkit (MECT) Version 2.1.1 Released
CMS is proud to announce the release of the Medicaid Enterprise Certification Toolkit (MECT) v2.1.1. This is a minor release of the toolkit to bring MECT in line with recent State Medicaid Directors Letters.
Highlights of the MECT v2.1.1 release include:
- Provided clarification for the role of the systems integrator
- Updated language in Section 1 of 04 MECT 2_1_1 Appendix C_Std IV&V Language around the use of the term “Department”
- Provided additional information to explain how states can provide evidence for not applicable criteria and for criteria that cover functionality being performed by a different module
Please refer to MECT 2.1.1 Welcome and Release Notes for detailed information about the changes available on https://www.medicaid.gov/medicaid/data-and-systems/mect/index.html. CMS is dedicated to keeping MECT current with all federal regulation and Medicaid priorities and will continue to publish updated versions to the MECT. It is recommended that states and vendors review and understand the latest guidance in the MECT to ensure compliance.
Please send questions about the new MECT 2.1.1 to: mmis_mes_certification@cms.hhs.gov
About the Medicaid Enterprise Certification Toolkit
The MECT was developed to assist states as they plan, develop, test and implement their Medicaid Management Information Systems (MMIS). The Toolkit has been updated to accommodate modular and agile development, refined certification criteria, a new approach to CMS-State partnership during MMIS development, and to reflect the latest regulations and guidance.
Updated toolkit information and training can be found here:
https://www.medicaid.gov/medicaid/data-and-systems/mect/index.html
Medicaid Enterprise Certification Toolkit (MECT) Highlight
Medicaid Enterprise Certification Roles, IV&V Contractor
The IV&V contractor represents the interests of CMS and,
as such, provides an independent and unbiased perspective on the progress of
MMIS development and the integrity and functionality of the system. CMS expects
that the IV&V contractor will participate in state SDLC gate reviews and
will inform CMS of significant risks or issues as the module(s)/system is
planned, developed, and deployed. To
ensure independence, the IV&V contractor must not report to the same agency
or department that oversees the Medicaid program. (For example, the
IV&V contract may be owned by the state’s auditor’s office or the state’s
department of treasury.) The IV&V contractor must not be the contractor
performing software testing.
According to 45 CFR § 95.626 (b) and (c),
(b)
Independent verification and validation efforts must be conducted by an
entity that is independent from the state (unless the state receives an
exception from the Department), and the entity selected must:
(1)
Develop a project work plan. The plan must be provided directly to the
Department at the same time it is given to the state.
(2)
Review and make recommendations on both the management of the project,
both state and vendor, and the technical aspects of the project. The IV&V
provider must give the results of its analysis directly to the federal agencies
that required the IV&V at the same time it reports to the state.
(3)
Consult with all stakeholders and assess the user involvement and buy-in
regarding system functionality and the system’s ability to support program
business needs.
(4)
Conduct an analysis of past project performance sufficient to identify
and make recommendations for improvement.
(5)
Provide risk management assessment and capacity planning services.
(6)
Develop performance metrics which allow tracking project completion
against milestones set by the state.
(c)
The acquisition document and contract for selecting the IV&V
provider (or similar documents, if IV&V services are provided by other
state agencies) must include requirements regarding the experience and skills
of the key personnel proposed for the IV&V analysis. The contract (or
similar document, if the IV&V services are provided by other state
agencies) must specify by name the key personnel who actually will work on the
project. The acquisition documents and contract for required IV&V services
must be submitted to the Department for prior written approval.
CMS has developed standard IV&V language to be included
in the state’s IV&V RFP and contract (or contract modification, if a
contract already exists) to ensure that the IV&V contract includes duties
that CMS expects of the contractor. The standard language can be found in the
toolkit appendices.
The IV&V contractor prepares Part 1 and the checklists
of the MMIS IV&V Progress Reports throughout the certification life cycle,
but, in particular, before certification milestone reviews. The IV&V
contractor reviews project and technical progress against the state’s baseline
plans and against requirements contained within the Medicaid Enterprise
Certification Checklists. The IV&V contractor delivers the MMIS IV&V
Progress Reports, including draft reports, to CMS and to the state
simultaneously.
For additional information, please review the following
resources:
Cohort Recap
This month, the MMIS Cohort moved forward in four interrelated
areas of system development with respect to enhancing Cohort states’ efforts in
collaboration and reuse:
- Transitioning a legacy system - An introductory meeting and discussion was held on the topic of transitioning a state legacy system to a modular one. The meeting was well attended, with most states present. An effort is being made to identify common concerns to help frame solutions moving forward. A second meeting is planned for early January.
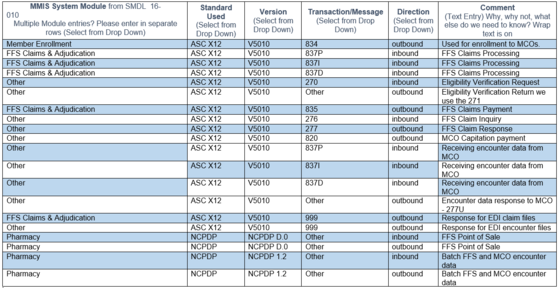
- MMIS data standards - A survey was sent to all
Cohort member states on the current status of MMIS data standards. Below is a
representative state’s reply. The full results will be distributed next month.
Since all states will be starting at different points, we hope this information
will help inform states’ data standard strategies as they transition their
systems.
- Prototype an MMIS module - A meeting was held
for states interested in an opportunity to prototype an MMIS module for
provider enrollment. We reviewed an opportunity on the table and discussed how
to consider this and various other approaches.
- Modular Systems Integration Framework - Hugh
Hale, CIO of the Tennessee Health Care Financing Administration, gave a
presentation on the state’s Modular Systems Integration Framework approach. The
discussion included experiences, helpful tips, and lessons learned.
 |
Appointment of the Medicaid Information Technology Architecture (MITA) Governance Board Members
|
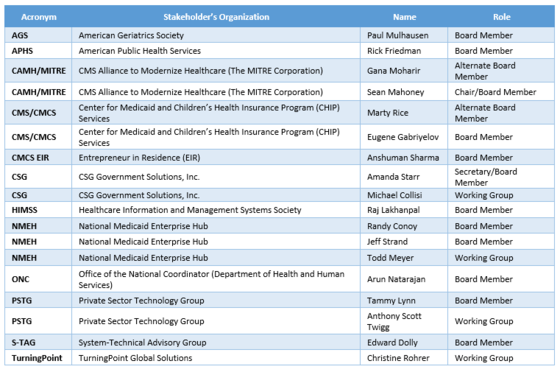
The Center for Medicaid and Children’s Health Insurance Program (CHIP) Services (CMCS) Data System Group Management announces the appointment of 12 new Medicaid Information Technology Architecture (MITA) Governance Board members, two alternates, and four working group members to serve two-year terms.
The MITA Governance Board maintains an operational focus as it leverages a broad range of stakeholder perspectives to provide strategic counsel to CMCS management about the MITA framework. Specifically, board members will identify MITA enhancement opportunities and direct the overall growth and evolution of the MITA framework. MITA enhancement opportunities are presented to CMCS management for priority approval.
The MITA Governance Board determines the best way to operationalize these enhancements using qualified resources (working groups) to direct and participate in priority projects based on subject matter expertise.
CMCS is very pleased to welcome these outstanding IT healthcare leaders to the MITA Governance Board. The breadth, depth, and diversity of their experience will strengthen the MITA framework for the future. Each board member has a reputation for collaborative leadership—a MITA value that the Centers for Medicare & Medicaid Services (CMS) supports.
For more information, contact the MITA Governance Board by email at mmis_mes_certification@cms.hhs.gov?subject=mitagovernance.
|
|
|
SHARE THE KNOWLEDGE! To be added to the MMIS Newsletter distribution list click here.
|