|
The leading body for maternity and newborn safety investigations in England |
|
|
A monthly bulletin for stakeholders, clinical and non-clinical staff working in maternity, neonatal care and patient safety.
|
|
MNSI celebrates first prize win at RCOG World Congress
Two MNSI staff members, Louise Wake and Jo Francis, were awarded first prize in the ‘best overall oral presentation’ category at the recent Royal College of Obstetricians and Gynaecologists (RCOG) World Congress. Their presentation, Improving Health Equity Analysis in Maternal Death Investigations, highlighted how MNSI’s innovative HEART and HEWS Health Equity Toolkit is supporting investigators to identify, record, and respond to health inequities in maternity and newborn care.
The HEART (Health Equity Assessment and Review Tool) and HEWS (Health Equity Warning Score) toolkit equips MNSI investigators with a structured way to explore how wider determinants of health such as ethnicity, language, deprivation, or access to care may have influenced the quality and safety of care. It helps ensure that equity considerations are embedded in every stage of MNSI’s investigation process, from information gathering to final analysis.
Louise and Jo’s presentation demonstrated how this approach places health equity at the centre of maternity and newborn safety investigations. By enabling teams to clearly map and describe how barriers to equitable care may have contributed to adverse outcomes, the toolkit supports actionable learning that promotes safer, fairer care for all women, birthing people, and babies.
Jo Francis said:
"We want to understand the root causes of unsafe care, especially where barriers to equity may have played a role. This toolkit helps us do that in a structured and consistent way, so that no one is left behind in efforts to improve maternity and newborn safety."
Louise Wake added:
"By enhancing how we analyse equity in these investigations, we hope to achieve real change in policy and practice, ultimately improving outcomes for families from all backgrounds.
“We are absolutely thrilled that our work has been recognised by the RCOG.”

|
|
MNSI’s three-year strategy development has now reached its halfway point. The discovery phase has been completed which included stakeholder interviews with families, NHS trusts, and national partners, as well as valuable feedback gathered through an NHS trust survey.
We want to extend our thanks to everyone who has contributed their time and insights, your input is invaluable in shaping the future of maternity and newborn safety investigations.
With this foundational work complete, the Programme is now focused on developing the emerging themes from the discovery phase into clear strategic priorities. These priorities will guide our work over the coming years, ensuring we continue to improve safety, equity, and thematic learning across maternity and newborn care.
Our strategy development will also be informed by recent national initiatives, including the 10-Year Health Plan for England and the Dash Review on patient safety.
We look forward to sharing further updates as the strategy takes shape.
|
|
|
A baby received an exchange blood transfusion. This is a specialist and complex procedure with associated risks (and is now infrequently performed in most neonatal units). During the exchange transfusion procedure, the baby’s condition deteriorated and they had a cardiac arrest, which was due to hypovolaemia as the incorrect infusion line had been used. The baby was later diagnosed with severe brain injury, meeting the criteria for MNSI investigation.
The procedure for transfusing donor blood involved the use of a multi-function, volumetric pump and a specific infusion line for use with blood. Pre-made procedure packs contained the incorrect infusion line for the administration of blood. The packs contained an infusion line for clear fluids, which has a much finer filter, with smaller holes, this means that red blood cells cannot effectively pass through the filter. For the volumetric pump used, the packaging of the different infusion lines differs in colour; the differences are less obvious without the packaging.[1] It was not recognised that the incorrect infusion line was being used.
Priming the infusion line took much longer than expected; visually blood was seen moving through the line which gave reassurance that the equipment was working as intended. During the procedure the volumetric infusion pump showed that the expected volume had been infused, which meant staff were not alerted that the baby was not receiving sufficient blood until after their condition deteriorated.
[1] This equipment issue has been reported to the MHRA via the Yellow Card scheme, in accordance with regulatory requirements for medical device safety.
|
|
- Does your local process ensure a repeat bilirubin is measured before starting the exchange transfusion to ensure that it is still required?
- Are all staff aware that infusion lines differ and know about the different filter characteristics?
- How are staff supported to recognise different infusion lines?
- Where equipment is collected into ‘packs’ for a procedure, how does the trust ensure the correct equipment is included?
- How do staff, of all levels of seniority, recognise and seek help when events are not progressing as expected? For example, how long the infusion line should take to prime and when should this trigger a review of the equipment being used?
- Does local simulation training include the use of the incorrect infusion line with expired blood, to demonstrate the impact of this on the procedure?
- How does the local system of recording and overseeing a baby’s observations support staff to recognise changes in their condition during the exchange transfusion?
- Does your local process for exchange transfusion include a role, focussed on oversight of the transfusion, to help recognise and respond to any deterioration, including stopping the procedure?
|
|
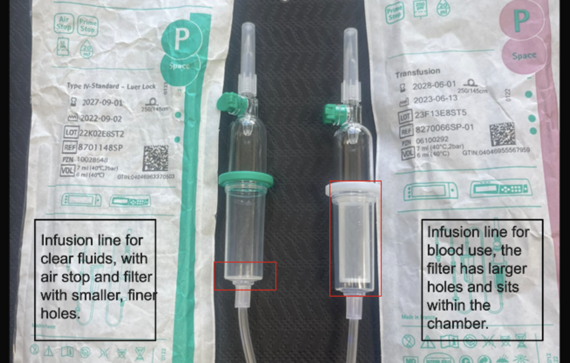 Image of clear fluid infusion line (left) and infusion line for use with blood (right):
MNSI has welcomed the recent publication of the Dash Review into patient safety across the health and care landscape and the NHS 10-Year Plan, both of which set out ambitious proposals to strengthen patient safety and learning across the health and care system.
The government’s 10-Year Health Plan’s commitment to making the NHS the safest and most equitable healthcare system in the world strongly aligns with MNSI’s purpose. The Plan, alongside the Secretary of State’s maternity care announcements in June 2025, signals a renewed national focus on tackling inequalities and improving outcomes for women, birthing people, and babies. The Dash Review outlines a clear vision for strengthening patient safety across the health and care landscape.
|
|

Our recent webinar series saw 600 maternity and newborn care professionals join the sessions, bringing the combined total for both webinar series to more than 1,000 participants.
We are pleased to see that these webinars have offered a valuable learning opportunity, with feedback from 68 attendees highlighting the impact of these sessions:
-
85% said they learnt something new
-
76% felt they could apply the learning immediately in their work
- and an impressive 90% agreed that the information shared could help improve patient safety.
Thank you so much to everyone who has taken part and contributed to these sessions.
We are in the process of planning for webinar series three and will share more details in due course. In the meantime, you can catch up on all the webinars on the MNSI website here.
As part of a national effort to improve how qualifying perinatal events are notified, NHS England is launching the Submit a Perinatal Event Notification (SPEN) portal, a unified system that will replace the separate reporting portals currently used by MNSI, MBRRACE-UK, and NHS Resolution.
The SPEN portal has been developed to streamline the reporting process, save time, and improve the accuracy of submitted data. By creating a single point of entry, SPEN allows information submitted for one organisation to be automatically shared with others, significantly reducing duplication. It also ensures that headline data feeds directly into the new Maternity Outcomes Signal System (MOSS), helping to identify safety concerns earlier and support national maternity and neonatal safety efforts.
What this means for you
MNSI’s current referral portal will remain in use during the transition period. However, once SPEN is fully implemented and all legacy cases are concluded, the MNSI portal will be retired.
For trusts participating in the SPEN Trial or early rollout waves:
- From your go-live date, all new MNSI referrals must be uploaded via the SPEN portal.
- Any new referrals submitted to the legacy MNSI system after your go-live date will not be processed and will be automatically removed.
- For existing referrals and ongoing investigations, please continue to use the MNSI legacy portal until the investigation is formally concluded.
For trusts not yet using SPEN:
- Please continue to submit referrals to MNSI via the existing portal as normal.
- You will receive further guidance and onboarding support before any changes to your submission process take effect.
MNSI is working closely with NHS England and other national partners to ensure this transition is smooth and fully supported. We will continue to share updates and provide assistance throughout the rollout.
For any queries about referrals during this transition or for support with your MNSI submission process, please contact MNSI_SPEN@mnsi.org.uk.
September
HSJ Patient Safety Congress, 15 - 16 September, Manchester
Baby Lifeline National Maternity Safety Conference, 25 September, Birmingham
November
Awareness Days
World Patient Safety Day, Wednesday 17 September 2025
Baby Loss Awareness Week, 9 - 15 October, 2025
|
|
|
|
|

