Better Tools to Combat the Opioid Crisis
On average, one Oregonian dies every three days due to the misuse of prescription opioids. Please take a moment to let that sink in—one Oregonian every three days.
In Oregon, 4,270 people were recently prescribed a dangerous combination of three drugs (opioids, benzos, and muscle relaxants) in the same month, which can be lethal if taken together. One Oregonian received a 1,545 days’ supply of zolpidem (which can be used as a date rape drug) from five separate prescribers in a single year. Shockingly, 148 Oregonians received controlled substance prescriptions from 30 or more separate prescribers and filled their prescriptions at 15 or more pharmacies within a three-year time frame.
These findings, and more, were revealed in the audit we released yesterday. It focused on Oregon’s response to the opioid crisis through the Oregon Health Authority (OHA)’s monitoring of prescription drugs. I encourage you to read the audit yourself, or you can watch the press conference held yesterday afternoon by the audit team.
 The opioid crisis affects all of us in one way or another, and it is our collective responsibility as Oregonians to take action.
Many of us have family or friends who have been victims of addiction. Some of you may have even battled it yourself. Even those who may not experience the heart-wrenching personal and emotional costs, they do pay the financial cost through increased taxes and insurance premiums from the ripple effects of this horrible crisis—health care, prisons, foster care, etc.
It is important to remember that opioids can be helpful in addressing pain with appropriate medical oversight, but they are also highly addictive. Dependence on prescription opioids can occur in less than a week, and taking a low dose prescription of an opioid for more than three months raises the risk of addiction 15-fold.
While some progress has been made recently, Oregon still prescribes opioids at a rate of 13% more than the U.S. average, and the U.S. prescribes more than other comparable countries.
The effects of the opioid crisis in Oregon are heartbreaking. We have the highest rate in the nation of seniors hospitalized for opioid-related issues such as overdose, abuse, and dependence. The median cost for each hospitalization due to opioids is $13,000. The state also has the sixth-highest percentage of teenage drug users.
In 2016, almost 500 pregnancies were complicated by maternal opioid use and 280 infants were born with Neonatal Abstinence Syndrome, or problems due to withdrawal from addictive substance exposure during pregnancy. From 2015 to 2017, 314 more children entered foster care due to a parent’s drug abuse.
Many opioid deaths are preventable, but our audit revealed that OHA has been trying to fight this crisis with one hand tied behind its back. We should learn from the experiences of other states and follow methods being successfully implemented across the nation.
An important tool that all 50 states use to help combat the opioid crisis is a Prescription Drug Monitoring Program (PDMP). PDMPs collect information on opioid and other controlled substance prescriptions directly from certain pharmacies to provide healthcare professionals with a patient’s prescription history. PDMPs also allow tracking of physician prescribing practices to help state authorities create informed guidelines and other efforts to improve addiction prevention and treatment.
Compared to other states, Oregon’s PDMP collects less information. It is used less effectively. It does not allow key players reasonable access to information.
Oregon lags behind neighboring states in implementing best practices, as you can see from the chart below:
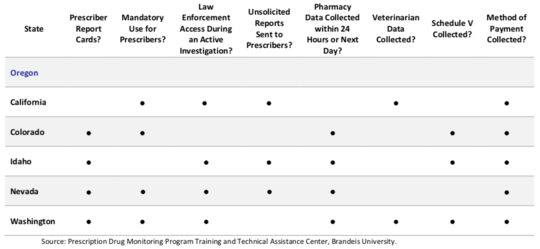 Many states produce report cards that give prescribers a tool to self-examine their behaviors and help positively influence their prescribing of controlled substances. Oregon does not.
Many states require all prescribers and pharmacies to participate in the PDMP program. Since Oregon does not, our PDMP lacks critical information. When prescribers don’t know a patient’s full prescription history, there is a higher risk of prescribing dangerous combinations of drugs.
For example, our data analysis revealed 4,270 people who were prescribed a dangerous combination of three drugs (opioids, benzos, and muscle relaxants) in the same month, which can be lethal when taken together. Many patients have reasonable need for these drugs separately and sometimes in different combinations, but there are very few reasons why a patient would be legitimately prescribed all three of these drugs at the same time. During a 36-month period, 864 people had all three—opioid, benzos, and muscle relaxants—for at least 10 months. These sorts of dangerous drug combinations can be reduced by better PDMP data collection and use.
In another example, we found troubling instances of potentially excessive quantities of zolpidem, which has been used as a date rape drug. One person received a 1,545 days’ supply of zolpidem from five different prescribers in a single year. Currently, OHA cannot share this data with law enforcement.
Using PDMP data, our audit team found numerous instances of potential “doctor shopping,” which occurs when a patient receives controlled substance prescriptions from multiple healthcare prescribers without the prescribers’ knowledge of the other prescriptions.
During the three-year period our team examined, the average person received controlled substance prescriptions from two different prescribers and filled their prescriptions at two different pharmacies. Shockingly, the audit identified 148 people who received controlled substance prescriptions from 30 or more different prescribers and filled their prescriptions at 15 or more pharmacies within our three-year time frame. In one of the most egregious cases, the person had 32 opioid prescriptions paid for by Medicaid. PDMP changes can help prevent this.
Another area of significant concern is that some types of pharmacies are excluded from the PDMP altogether. Over the course of one month, an individual was prescribed 354 tablets of oxycodone and 171 tablets of clonazepam by three different doctors. Because some of these prescriptions were filled at exempt pharmacies, they were not included in the patient’s PDMP prescription history.
There are many other disturbing findings in this audit. Oregon can and must do better.
Many opioid deaths are preventable. This audit provides a roadmap of solutions to help save lives.
|


