|
|
Oregon’s long-term care facilities face a substantial risk of spreading respiratory illness due to close-quarter living conditions and the health vulnerabilities of residents. Between September 2023 and August 2024, more than 960 outbreaks of respiratory viruses were reported in these facilities. Many visitors and staff enter and leave these buildings daily, which increases the chance of infection. While improving air quality by upgrading HVAC systems or opening windows can help, these solutions are often expensive or impractical. For example, in memory-care settings, opening windows can pose a safety risk for residents.
To tackle this issue, the Oregon Health Authority’s (OHA’s) Healthcare Acquired Infections (HAI) Program provided long-term care facilities with High-Efficiency Particulate Air (HEPA) units and replacement filters at no charge. These HEPA filters improve indoor air quality by trapping harmful particles, including viruses, which helps protect both residents and staff. The program targeted nursing facilities, assisted living facilities, and residential care homes across Oregon ahead of the 2024–25 respiratory illness season.
The Medify Air MA-40 model was chosen for its size, making it ideal for both resident rooms and shared spaces like dining areas and staff rooms. Each facility received a one-year supply of medical-grade replacement filters, which remove 99.9% of harmful particles. Between March and May 2024, over 500 long-term care facilities in Oregon received HEPA units, with 71% of nursing facilities now equipped.
These HEPA units are a major step toward improving air quality and protecting vulnerable residents in these congregate settings. We’re proud of this initiative and its anticipated impact on health and safety for Oregon’s long-term care communities.
For questions contact Bailey Weissenfels.
|
|
Infections Insights
 |
|
Check out the newest @CDCProjectFirstline micro-learn training on what to do when you see a rash. Train your team to recognize infection risks and stop the spread of germs. |

- As the fall respiratory virus season arrives, stay up to date with COVID-19, Flu and RSV trends by visiting OHA’s dashboards.
- Oregon continues to see low influenza vaccination rates among health care personnel following significant drops during the COVID-19 pandemic, according to new OHA data. The Healthcare Worker Influenza Vaccination Dashboard shows that 61% of the state’s health care workers from all facility types were vaccinated among those eligible during the 2023–2024 flu season.
- Beginning September 30, the National Healthcare Safety Network (NHSN) updates its COVID-19 vaccination reporting to reflect the new definition of “up to date.” Residents and staff should be considered up to date if they received the 2024–2025 COVID-19 vaccine; or the 2023–2024 COVID-19 vaccine in the last two months. Residents and staff who received a 2023–2024 COVID-19 vaccine more than two months ago should no longer be considered up to date. Refer to NHSN for additional guidance.
- We want to recognize the great antimicrobial stewardship work happening in Oregon’s acute-care and critical-access hospitals. Apply to Oregon’s Antimicrobial Stewardship (AMS) Honor Roll, and tune in to our special edition newsletter in November to meet our first honorees! For more information visit our webpage or email us.
- Eligible acute-care and critical-access hospitals have two module options for reporting relevant data to the NHSN antimicrobial use and resistance (AUR) Module to meet the CMS requirements for calendar year 2024. Find more information about these modules in the NHSN Newsletterand AUR Reporting FAQs.
- OHA recommends that Oregon hospitals and ventilator-capable skilled nursing facilities screen on admission for Candida auris and carbapenemase-producing organisms (CPOs), in patients who in the past 12 months:
- Spent the night in a healthcare facility (hospital or long-term care) outside of Oregon or
- Had outpatient surgery or hemodialysis outside the US or Canada.
Testing is provided at no cost to facilities. Contact us to get started.
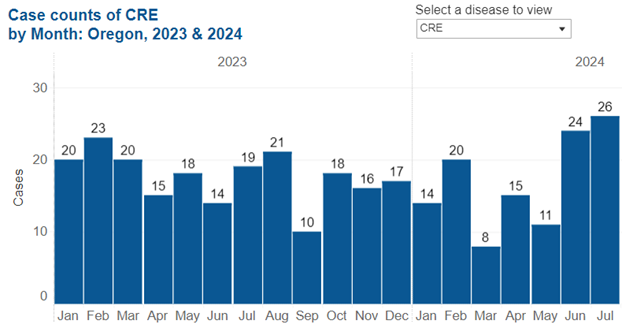
- Keep track of carbapenem-resistant Enterobacterales (CRE) cases using OHA's Disease Surveillance Report. Explore this and other diseases, like West Nile virus, Lyme disease, and Mpox.
|
|
-
International Infection Prevention Week is October 15–21, 2024. Infection Preventionists (IPs) play a crucial role in keeping patients safe and healthy—protecting them from surges in healthcare-associated infections and so many other infectious threats.
-
National Pharmacy Week takes place from October 20–26, 2024. Pharmacists are medication experts and play an essential role in antibiotic stewardship. They are a great resource for questions about antibiotics and medication disposal. Remember to #ThankAPharmacist to recognize all the work they do in keeping us healthy.
-
U.S. Antibiotic Awareness Week (USAAW) highlights the significance of proper antibiotic use and the dangers posed by antimicrobial resistance. This year, USAAW will take place November 18-24. The following resources provide messages and materials you can share with your community and partners.
- Copy and share sample social media messages and graphics. #AntimicrobialResistance #USAAW24
- Promote resources with important information about appropriate antibiotic and antifungal use, antibiotic stewardship, and antimicrobial resistance.
- Stay tuned for the special edition of the HAI Chronicle in honor of USAAW.
|
|
|
Get to know the exceptional members of the HAI team. This month, we’re excited to feature Rachel Geissler (on the left below), a dedicated infection preventionist on the HAI team, serving regions 3 (Lane, Douglas, Curry, and Coos counties) and 5 (Jackson and Josephine counties), as well as Deschutes County.

With a passion for public health, Rachel supports healthcare facilities to strengthen infection prevention and improve patient outcomes. Rachel earned her BSN from Oregon Health & Science University’s School of Nursing and began her nursing career in the emergency room. However, she soon found that hospital nursing wasn’t for her. Rachel transitioned to Home Health, where she discovered a passion for chronic wound management. After briefly returning to hospital leadership, Rachel found her true calling in infection prevention (IP) at the start of the COVID-19 pandemic—a role that sparked her nursing passion. She earned her Certification in Infection Control in 2023, further deepening her expertise.
Rachel’s primary role on the HAI team is to provide consults, learning sessions, and ongoing infection prevention support to healthcare workers in her regions. She works with a wide range of organizations, from long-term care facilities and outpatient clinics to non-traditional healthcare settings that serve people experiencing homelessness. One of her proudest contributions is hosting monthly virtual IP community-building sessions, where infection prevention professionals can come together, share experiences, and ask questions in an informal setting. Rachel is also helping develop a consult-tracking tool that will streamline infection prevention recommendations and measure progress over time.
In her free time, Rachel enjoys running trails, doing restoration work, reading, spending time with her dog, and taking on home projects with her husband.
Two quotes that inspire Rachel and adorn her workspace are: “No two people ever read the same book” and “Never buy anything from a man selling fear.” Though she doesn’t remember who said them, these reminders keep her grounded as she tackles infection prevention challenges.
|
 |
In September, CDC published the Core Elements of Hospital Diagnostic Excellence Programs, which outline strategies to address diagnostic errors, missed diagnoses, and diagnostic stewardship. Because diagnostic tests are crucial for patient diagnosis, they can greatly influence antibiotic prescribing.
What is Diagnostic Stewardship?
Effective diagnostic stewardship means choosing the right tests for the right patient, at the right time to provide the right treatment. This principle is important to antibiotic stewardship, as an incorrect diagnosis can lead to prescribing an antibiotic when one is not needed, or to a failure to prescribe an antibiotic when one is needed, both of which can harm patients. The table below illustrates some examples of the relationship between diagnostic stewardship and antibiotic stewardship.
|
|
Stewardship Questions
|
Examples Elements of Diagnostic Excellence
|
|
1. Differential Diagnosis
|
|
Antibiotic Stewardship
|
Does my patient have an infection that requires antibiotics?
|
Remove any automatic orders for diagnostic tests.
Inform clinicians about test choice and interpretation.
Require clinicians to document symptoms or treatment indications when ordering urine cultures.
|
|
Diagnostic Stewardship
|
Should I order a test to determine if my patient has an infection? If so, what test is appropriate?
Will the test change my treatment decision?
|
|
2. Empiric treatment and appropriate cultures
|
|
Antibiotic Stewardship
|
Have I ordered appropriate cultures? What empiric therapy is appropriate?
|
Focus on proper specimen collection and handling to prevent errors.
Educate staff on proper specimen-collection technique.
|
|
Diagnostic Stewardship
|
Was the specimen appropriately collected and stored?
How should the specimen be tested?
|
|
3. Refine diagnosis and treatment
|
|
Antibiotic Stewardship
|
Can I stop antibiotics?
Am I using the narrowest-spectrum antibiotic that will do the job?
|
Implement changes to test reporting to reduce erroneous diagnoses and subsequent overtreatment (e.g., when multiple organisms in urine culture are found, the report notes "likely contamination")
Selective or cascaded susceptibility reporting can prevent prescribers from using high-risk, excessively broad-spectrum antibiotics.
|
|
Diagnostic Stewardship
|
What do the test results tell me about what I should do for my patient?
Is there evidence of an infection?
Does the test inform as to which antibiotics will be effective?
|
|
4. Final diagnosis and treatment
|
|
Antibiotic Stewardship
|
What duration of antibiotic therapy is needed for my patient’s diagnosis?
|
Provide clinicians with easy access to reference materials, checklists, and resources for diagnosis (testingwisely.com and Global Knowledge Sharing Platform for Patient Safety)
|
|
Diagnostic Stewardship
|
Are there follow-up diagnostic tests I should or should not perform?
|
Adapted from the Society for Healthcare Epidemiology of America (SHEA) Position Paper Improving antimicrobial use through better diagnosis: The relationship between diagnostic stewardship and antimicrobial stewardship and the Agency for Healthcare Research and Quality’s (AHRQ’s) Four Moments of Antibiotic Decision Making.
|
|
I’m a healthcare worker. How soon after I have COVID-19 can I return to work?
The time it takes to return to work after having COVID-19 depends on how severe your illness was and whether you are immunocompromised. You can read the full CDC guidance for healthcare workers, but below is a simplified overview. Follow your facility’s policy, which may be different.
-
No symptoms (not immunocompromised): You can return after at least 7 days if you test negative within 48 hours of returning (or 10 days if no test or positive test at day 5–7).
-
Mild to moderate illness (not immunocompromised): You can return after at least 7 days if you test negative within 48 hours of returning (or 10 days if no test or a positive test at day 5–7), have been fever-free for 24 hours without medication, and your symptoms have improved.
-
Severe to critical illness (not immunocompromised): You may return after 10–20 days, depending on your recovery, if fever-free for 24 hours without medication and symptoms have improved.
-
Moderately to severely immunocompromised: You may need more time before returning. Consult your healthcare provider and consider testing negative with two tests, 48 hours apart.
CDC Viral Respiratory Pathogens Toolkit for Nursing Homes
At-A-Glance Infection Control for Respiratory Pathogens
|
|

Sign up for our newsletter to receive regular updates, explore new resources added to our website, and reach out to us with any questions or ideas you'd like to see in future newsletters. Let us know!
-
Sign up for our newsletter.
-
Share your feedback/suggestions/topics for future newsletters.
- Visit our website.
|
|
|
|
Oregon Health Authority works to transform the health care system in Oregon by lowering and containing costs, improving quality and increasing access to care to improve the lifelong health of Oregonians. OHA is overseen by the nine-member citizen Oregon Health Policy Board working toward comprehensive health reform in our state.
The HAI program within the OHA Public Health Division is dedicated to preventing and containing healthcare associated infections (HAIs) and addressing the growing challenge of antimicrobial resistance (AR). Through initiatives such as the Antimicrobial Resistance Laboratory Network (AR Lab Network) and the National Healthcare Safety Network (NHSN), we are bolstering our ability to detect and respond to antibiotic resistance while strengthening the nation's most widely used HAI tracking system. We also focus on antibiotic stewardship to improve the appropriate use of antibiotics, and we provide comprehensive infection prevention and control (IPC) education and training to equip the health care workforce with the necessary skills. Our team further offers IPC consultations to health care facilities throughout the state, providing expert guidance and support in implementing effective infection prevention strategies and responding to outbreaks. Together, we are committed to enhancing patient safety and reducing the impact of HAIs and antimicrobial resistance.
|
|
|
|
|