|
Members of the Oregon
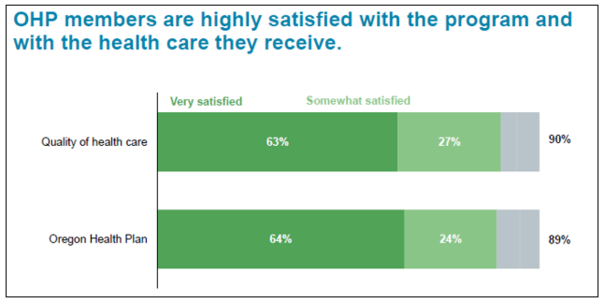
Health Plan (OHP) are highly satisfied with the care they receive, trust the
state’s Medicaid program for information about their health, and support proposed
changes in coordinated care contracts known as CCO 2.0.
That's according to a survey
by DHM Research, which conducted telephone interviews with 401 OHP members in
late August. Interviewers spoke to OHP members whose primary languages were
English, Spanish, Russian and Vietnamese. The survey found few significant
differences of opinion among respondents based on language, region or other factors
such as gender, age, race or ethnicity.
DHM presented the
findings to the Oregon Health Policy Board Sept. 11. The board received draft
recommendations for the CCO 2.0 contracts and will approve final changes at its
meeting October 15.
Some of the results:
-
Satisfaction with OHP: 90 percent of respondents were
satisfied with OHP and the care they receive through the plan. (Sixty-three
percent were very satisfied.)
-
Satisfaction with CCOs: 78 percent who were familiar with
coordinated care organizations were satisfied with CCOs. (Fifty-five percent
were very satisfied.)
-
Ways to improve care: When asked what they would change, one-third would
not change OHP. For those who offered responses, the top changes were: expand
coverage (23 percent), reduce wait times for care and customer service (12
percent) and improve access to and choice of providers (10 percent).
OHP members showed
support for the major proposals to change CCO contracts:
-
Improve access to behavioral health services: 76 percent supported.
-
Address social factors that affect health: 83 percent supported.
-
Contain costs: 50 percent supported.
-
Pay providers to improve member health: 48 percent supported,
42 percent opposed.
-
Transparency and representation: 63 percent agreed "having
more members help make decisions about OHP would improve your health care
experience."
The survey has a margin
of error of plus or minus 4.9 percent.
Governor
Kate Brown released her health
care strategy, which would build on Oregon’s 94 percent rate of health
coverage, sustain health transformation, and hold down health care costs. The
plan outlines eight health care priorities:
- Ensure Oregonians’ access to health insurance
coverage.
- Improve overall health outcomes
through CCO 2.0.
- Control long-term cost growth in
health care spending.
- Use reinsurance to keep rates
affordable in the private market.
- Increase investments in mental health
and addiction prevention and treatment.
- Modernize public health.
- Increase capacity, retention, and
diversity in Oregon’s health care workforce.
- Create better health through good jobs.
You can read
Governor Brown’s plan “Health Care for All” here.

The Oregon Health
Authority values transparency, accountability, and the wise use of public
resources. In an effort to increase transparency, OHA Director Patrick Allen
will share his weekly
calendar, after redacting private information. Director Allen further
believes that sharing his appointments calendar will help him take a step back
from his daily meetings and ensure he is meeting with and listening to a wide
variety of people, partners, and stakeholders. You can view it on the OHA
website.

The Oregon
Health Policy Board (OHPB) will receive the final policy recommendations for
CCO 2.0 at its meeting on
October 15. The proposals will define the requirements OHA includes in the
next contracts it issues to coordinated care organizations (CCOs), beginning in
2020. OHA will issue a request for proposals in early 2019.
The health
policy board reviewed a draft
CCO 2.0 policy report at its September meeting. The draft report describes
how CCO 2.0 would advance health transformation and tackle Oregon’s biggest
health problems through four major priorities:
-
Improve behavioral health and
streamline access to care for consumers by a) improving gaps in care between doctors and behavioral
health providers, b) making CCOs more accountable for behavioral health
benefits and c) expanding and diversifying networks of care in underserved
areas.
-
Address social factors that affect
health and reduce health disparities by giving CCOs more financial incentives to target upstream
problems (such as poor housing, food insecurity and lack of transportation)
that contribute to poor health. Encourage CCOs to improve coordination with
local public health departments and non-profit partners.
-
Increase value and pay for
performance by
setting statewide and CCO targets for provider payments that are based on
outcomes, not volume. Increase the amount of value-based payments across
state-managed public employee and educator health plans, as well as commercial plans.
-
Maintain sustainable cost growth and encourage financial transparency by rewarding efficient care
delivery, high-value clinical care and cost reduction.
Process for selecting CCOs
CCOs
will be selected through a request for application (RFA) process. Applications
will be accepted from entities with an existing Oregon “footprint.” Current
CCOs may remain in their service area or apply for the larger region in which
their service area resides. Applicants may also apply for more than one region.
End of CCO 2.0 public engagement
The October
OHPB meeting will conclude a two-year public engagement process that shaped the
next stage in the evolution of Oregon’s innovative coordinated care system, and
the terms of the next five-year CCO contracts. Throughout the process, the
policy board and OHA leaders have heard from hundreds of people across Oregon, including
OHP members. You can review CCO 2.0 proposals, public input and provide
additional comments prior to the deadline at the CCO 2.0 web page.
Since
Oregon implemented the Affordable Care Act (ACA) in 2014, more than 340,000
Oregonians have gained health insurance. Today, 94 percent (3.7 million
Oregonians) have coverage.
That
puts Oregon's uninsurance rate at 6.8
percent, compared to the national uninsurance rate of 8.7 percent, according
the U.S. Census Bureau’s latest American Community Survey (ACS).
This
new report comes on the heels of the state-based Oregon Health Insurance Survey
(OHIS), which pegged the uninsurance rate at 6.2 percent. The ACS and OHIS coverage rates vary slightly
due to differences in methodology. OHIS includes
more detailed information on demographics, access, use of services, cost of
care, and health status, and better represents minority groups in the state.
Oregon uses the ACS data to compare itself with other states and the national
average.
More people could be covered,
according to the OHIS Uninsurance
Fact Sheet. In fact, more than eight in 10 children, and
adults under age 65 who lacked coverage, are eligible for the Oregon Health
Plan (OHP) or financial assistance to reduce commercial health insurance
premium costs.
The top three reasons Oregonians cited
for not being covered by OHP were: concerned about high costs of coverage (44
percent); make too much money to be eligible (36 percent); and concerned about
quality of care (21 percent).
There
are no premium costs or deductibles for OHP's comprehensive benefit package of
medical, behavioral health and oral health care. Children and adults who
qualify for coverage under the Oregon Health Plan can apply any time during the
year. Oregonians can find more information about coverage available to them at OregonHealthCare.gov.

The Oregon Health Authority
welcomes Angie Allbee and Annaliese Dolph, the newest members of the Government
Relations team in the External Relations Division.
Angie
Allbee will support the Public Health Division. Angie joins OHA
after working as legislative liaison for the Oregon Department of Human
Services (DHS) for the past four legislative sessions. Prior to DHS Angie
worked for the Oregon Criminal Justice Commission, the Legislature's House
Majority Office, and for an Oregon state representative. Angie received her
Executive Master of Public Administration degree from Portland State
University’s Mark O. Hatfield School of Government.
|

Annaliese Dolph will support behavioral health. Annaliese is
an attorney who has more than a decade of experience in health policy. She has worked
for the National Multiple Sclerosis Society, various nonprofit organizations in
North Carolina, with an emphasis on behavioral health. Annaliese
has a Bachelor of Science from the University of Michigan and a Juris Doctorate
from the Santa Clara University School of Law.
Jeanette
Taylor will continue to support Medicaid policies and the Office
of Equity and Inclusion.
Two OHA staff are on job
rotations to join ombudsperson Ellen Pinney in the expanded program to better
serve Oregon Health Plan members with difficult or challenges cases.
|

Libbie
Rascon is on
rotation from her role as coordinator for the Office of Consumer Activities in
Health Systems Division's Behavioral Health program. In the role of an
ombudsperson, Libbie will apply her background in past government work,
business management, communications and her subject matter expertise in mental
health and addiction consumer voice. Libbie identifies as an ex-patient,
consumer survivor and person of lived experience (PLE). Her serving as a peer
support specialist (PSS) in the expanded Ombuds office will further enhance
OHA’s dedication to diversity and health integration.
|

Diane
St. Denis is on rotation from her role as a training and development
specialist in HSD Provider Services. As an ombudsperson, Diana will bring her
experience working with the Client Services Unit handling client calls. She
will be handling individual client cases, creating and improving educational
and resource materials for the recently created OHA Ombuds Program file on the
I Drive, and working with the Complaint Resolution Team (CRT) in the DHS Member
Services Client Services Unit to improve cross-agency ability to track client
calls and responses.
|

|

