|
Chronic kidney disease (CKD) is a progressive loss of kidney function, usually due to a decrease in functioning nephrons. Each kidney has about 1 million nephrons, such a large reserve can make slow, progressive loss unnoticeable until significant damage has occurred. CKD can involve reduced kidney function, indicated by low eGFR, and/or kidney damage indicated by appearance of albuminuria.
CKD in Montana & the USA
- Diabetes and hypertension are the leading causes
- 10% of Montana adults have diabetes
- 54.4% of Montana adults over age 65 have hypertension
- 15% of American adults have CKD
- Approximately 1 in 3 people with diabetes and 1 in 5 with hypertension have CKD
- 1 in 2 people with reduced kidney function, not on dialysis, don’t know they have it until function is severely compromised.
- Native Americans, African Americans, and Asian Americans have a higher incidence of end stage renal disease compared to Caucasians.
- CKD is often present at diagnosis in type 2 diabetes
- In people with diabetes, the presence of albuminuria even with normal kidney function, is associated with cardiovascular disease, CKD progression, and mortality.
 Graphic Source: The Change Package -check it out for more great information!
Screening for CKD
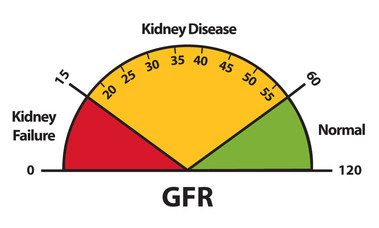
Estimated GFR or eGFR is the preferred method for quantifying kidney function. It varies by age, sex, and body size and declines with age. Normal eGFR is ≥ 90 ml/min/1.73m²
- The CKD-EPI Creatinine Equation is now the preferred method of calculating eGFR
The urine albumin to creatinine ratio (UACR) is used to describe the severity of kidney damage
- Done with a spot urine sample (not dipstick)
- A value of < 30 mg/g indicates normal or mildly increased albuminuria
- 30-300 mg/g is moderately increased (microalbuminuria)
- Greater than 300mg/g is severely increased (macroalbuminuria)
 Click this photo from the NIDDK to see great ways to explain CKD.
Recommendations
Did you know Renin-Angiotensin-Aldosterone System (RAAS) drugs are first-line agents at slowing the progression of CKD?
We can all be proactive in preventing the onset and slowing the progression of CKD by focusing on our diabetes and hypertension patients. Read more to learn how.
Pharmacists can help
Ensure:
The diagnosis of CKD, if applicable, is on your medication profiles and that patients are adherent to necessary medications.
Patients are treated for cardiovascular risk reduction with statins if indicated.
You have conversations with and educate patients identified with CKD.
Encourage:
Patients to “know their numbers” (eGFR and UACR or stage of CKD) so you can competently assess their medication regimens.
Regular BP monitoring with a validated electronic device.
Monitor:
Progression and stress importance of regular appointments (once or twice yearly) to have renal function tests done.
For drug interactions and renal dosing recommendations
Consider:
If medication therapies are correct and avoid those that cause acute kidney injury (e.g. NSAIDs).
Referring to a dietitian and/or certified Diabetes Care and Education Specialist
References
National Kidney Foundation Accessed 10/19/20 https://education.kidney.org/
NIDDK Accessed 10/16/20 https://www.niddk.nih.gov/health-information/professionals/education-cme/chronic-kidney-disease-management-pharmacists
American Diabetes Association Accessed 10/17/20 https://professional.diabetes.org/content-page/practice-guidelines-resources
Using Glucose Lowering Medication in People with Diabetes and CKD ADCES 2020 8/13/20
Please share and encourage colleagues to subscribe!
|

