
Ask the Expert: Cancer Screening
We asked our COE subject matter expert, Dr. Ann Settgast, to gain some insight into this issue.
Dr. Settgast completed her Internal Medicine residency at the University of Minnesota and after that obtained her diploma in Tropical Medicine and Hygiene from the Liverpool School of Tropical Medicine. Her international experience has included work or training in Ethiopia, Uganda, Tanzania, Laos, India, and the Dominican Republic.
Since 2006 she has practiced as a primary care general internist at the HealthPartners Center for International Health, where she has the privilege of caring for a largely refugee and immigrant patient population.
What do clinicians need to know about cancer screening for refugees?
Clinicians need to be aware that immigrants experience unique cancer risks and disparities in cancer screening in the U.S. Many barriers are responsible for the disparities, including, but not limited to, potential uninsurance/underinsurance or lack of a usual source of care; language and transportation barriers; and unawareness of the value of screening due to lack of prior access to cancer screening and/or lack of symptoms. Longer duration of residence in the U.S. correlates with improved screening rates.
What prevalence differences exist in refugee populations?
Many immigrants face elevated risks of infection-attributable cancers based on their country of origin. While formal screening guidelines for many of these cancers (e.g., stomach, gallbladder, bladder, nasopharyngeal) do not exist, it is important for providers caring for populations with increased risk to have familiarity with these cancers so that they have an increased index of clinical suspicion when needed.
How do recommendations for cancer screening in refugees differ from the U.S. preventative services task force guidelines?
Formal screening guidelines for hepatocellular cancer do exist in patients with chronic hepatitis B. Therefore, hepatitis B screening for immigrant patients who come from countries of >2% prevalence is an important first step in identifying those who will benefit from screening for this important infection-attributable cancer.
What are some infectious and environmental exposures you consider when thinking about cancer screening in refugees?
In terms of the "regular cancers" for which U.S. clinicians are accustomed to screening, there are a few nuances that are helpful to remember.
|
- For patients whose biological age differs from their "chart age," it is important to use the true biological age when making screening decisions.
- Special attention needs to be paid to women >65 in regard to cervical cancer screening. U.S. guidelines allow screening to cease at age 65 in women with history of prior normal screening. However, immigrant and refugee women are far more likely to be underscreened or never screened than their U.S.-born counterparts. Therefore, continuation of screening past age 65 for recently arrived women will often be needed.
- In women with type III FGC (infibulation) before their sexual debut (with no history of any form of sexual activity), cervical cancer screening is generally anatomically infeasible, may be traumatic, and fails to provide health benefit.
Cancer screening was just updated as a component of the domestic medical exam (DME). Do you have recommendations for the implementation of this guidance?
I think the DME can provide an opportunity for introduction to cancer screening, and in some cases implementation may be possible. For many immigrant patients, cancer screening will be a novel and foreign concept, and substantial education may be required. One of the keys to cancer screening success is the development of rapport and relationship with patients. This requires time and multiple visits, which puts the DME at a disadvantage in regard to the actual implementation of cancer screening. In the event you are the clinician conducting the DME but not the primary care provider, it is helpful to document that you discussed and introduced the concept of screening, in addition to the U.S. recommendations and norms around screening.
What key components should clinicians cover during education with their patients and during handoffs with primary care?
I think this totally depends on the situation. For example, if you are seeing a new arrival for the second DME visit and they've newly been diagnosed with uncontrolled diabetes, LTBI, and chronic hepatitis B, and they also happen to have not yet attained stable housing and the kids are not yet in school, there is no chance that you will even mention the idea of cancer screening. It is going to be at least #10 on your priority list. In this event, it is acceptable to refer refugees to primary care providers for cancer screening visits since cancer screening may require longer-term follow-up and coordination. However, if you are seeing someone who is completely healthy, has not had any chronic illness uncovered in their DME labs, and is adjusting well to their new life here, then discussing cancer screening may be feasible and appropriate at the DME visit.
Cancer screening resources:
- For clinicians:
- Translated resources for newcomers:
- Cancer Screening Publications
- Payton, C., Kvaratskhelia, N., Chalfin, M., Deffler, J., & Altshuler, M. (2025). Cervical, Breast, and Colorectal Cancer Screening Outcomes Among Refugees in Philadelphia, Pennsylvania. Journal of immigrant and minority health, 27(3), 480–488. doi:10.1007/s10903-025-01685-y
- Walker, P. F., Settgast, A., & DeSilva, M. B. (2022). Cancer Screening in Refugees and Immigrants: A Global Perspective. The American journal of tropical medicine and hygiene, 106(6), 1593–1600. doi:10.4269/ajtmh.21-0692
Newcomer Health Clinical FAQs
The Newcomer Health Clinical FAQs portal provides additional clinical information to clinicians and public health professionals working with newcomers. These commonly asked questions supplement the information found in CDC: Refugee Health Domestic Guidance, UpToDate, and other clinical guidance resources. Each FAQ includes a high-level response plus additional resources and citations.
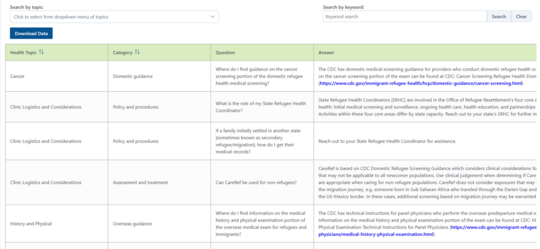
Can't find what you're looking for?
If you can’t find what you’re looking or have a need for technical assistance in your practice to care for newcomers, please submit your question to MN COE at MNCOENewcomerHealth@state.mn.us. Subject matter experts are available to help answer your technical assistance requests!
The technical assistance is for non-urgent questions regarding newcomer health, the domestic medical exam or screening guidance. Please only send de-identified cases and questions, to preserve all patient privacy and comply with HIPAA standards. Your request will be answered in 5-7 business days after being triaged and sent to one of the providers in our MN COE network, or one of their colleagues, if there is a need for additional specialized expertise.
Spotlight: Haitian Health Profile
The latest installment in our Haitian collection is the Haitian Newcomer Health Profile. As with our other health profiles, here you can find an in-depth narrative that discusses the health and culture of Haitians both in Haiti and after resettling in the U.S.
This health profile is informed by a comprehensive literature review and an MN COE-led analysis of data from five U.S. state refugee health programs.
- From October 2021 to September 2024, these programs were notified of 2,368 Haitian arrivals eligible for benefits from the Office of Refugee Resettlement (ORR), including Haitians in removal proceedings, with pending asylum applications, or with humanitarian parole.
- Among the 2,368 Haitian arrivals in this analysis, 1,488 (63%) received either a full or partial domestic medical exam (DME), and results were reported to the respective state refugee health program.
Hepatitis B Prevention Toolkit
The Migration Health Initiative released a Hepatitis B Dialogue Guide that supports hepatitis B screening and vaccine uptake in refugee, immigrant, and migrant communities. This resource equips providers with the tools they need to close critical gaps in hepatitis B prevention and care.
Stay up to date on the latest publications
Take a moment and review some recent publications on newcomer health:
- Ali, A., Elgharabawi, O., Hanson, J. L., Madigan, T., & Ferdjallah, A. (2026). Behind the splenomegaly: a parasitic twist in siblings with beta thalassemia trait. BMC pediatrics, 26(1), 264. doi:10.1186/s12887-026-06564-5
- Jung, E., Black, C., Placencio-Castro, M., Chamlagai, L., Osman, R., Hoffman, M., Beardslee, W., & Betancourt, T. S. (2026). Delivering a family-based child mental health promotion program among two resettled refugee communities during the COVID-19 pandemic: Lessons learned in a hybrid type II implementation-effectiveness randomized controlled trial. American journal of community psychology, 77(1-2), 231–247. doi:10.1002/ajcp.70021
- Um, M. Y., Kim, Y. K., Maleku, A., Baccam, Z., Abdullah, S., Shahin, J., Hesswany, A., Taknan, T., Sheikh, M., & Mulongo, P. (2026). Social support, social networks, and mental health of six refugee subgroups in Arizona: Findings from a pilot study. PLOS mental health, 3(2), e0000553. doi:10.1371/journal.pmen.0000553
- Alemi, Q., Todd Hesham, H., Cook, J., Naderi, W., & Afif, S. (2026). The Impact of a Culturally Adapted Patient Navigator-Led Telehealth Program for Displaced Afghans' Mental Health. Journal of immigrant and minority health, 28(1), 42–48. doi:10.1007/s10903-025-01758-y
The International Refugee and Migration Health Conference is just around the corner…
The Society of Refugee Healthcare Providers’ annual conference, the International Refugee and Migration Health Conference (formerly known as the North American Refugee Health Conference, or NARHC), will be held June 26-28, 2026, in San Diego, California.
Read about their incredible lineup of distinguished conference speakers and don’t forget to register!

|


