|
MIIC News Flash: Fall 2025 |
|
|
View this as a webpage
November 3, 2025
Data privacy, security, and quality are top priorities for the Minnesota Immunization Information Connection (MIIC). Organizations must complete and submit a MIIC Data Use Agreement (DUA) before being set up in MIIC. As a commitment to upholding these priorities, while participating in MIIC organizations must complete a new DUA every three years. The next time you update your DUA; you may notice some slight changes. The changes include:
- Defining “MIIC Manager,” an individual referenced in several terms of the DUA.
- Adding an “Unallowable Uses of MIIC” section to add clarity around how organizations can and cannot use MIIC.
- Slight language changes for clarity.
- Adding new DUA “terms”, including:
- All authorized users must complete privacy and security training, including training on proper MIIC use, before being granted access.
- The Organization must cooperate with MDH in any audits, monitoring, or investigations related to MIIC access and use.
- MIIC users should be assigned minimum level of access necessary to perform their job duties. Learn more about user roles at Managing Users (PDF).
These changes went live on Sept. 30. Review them at Data Use Agreement for Participating in the Minnesota Immunization Information Connection (MIIC) (PDF) and contact Health.MIICHelp@state.mn.us if you have questions about the updates.
All provider organizations and MIIC users should routinely review the Allowable uses of MIIC. Your MIIC access should not be used to assess a person’s immunization status for employment purposes. This includes verifying immunization status when those immunizations are required for employment. One exception is when individual services are being provided to the employee by health care organizations or in health care settings, such as reporting to MIIC an immunization your organization administered. A person’s written or verbal consent is not sufficient to authorize an organization or MIIC user to access immunization data for employment purposes. Organizations who require their employees to share proof of vaccination have several options.
VaxCheck
Organizations who request influenza and/or COVID-19 immunization information for their employees can consider participating in VaxCheck. It is a tool designed to collect electronic consent from employees to allow the Minnesota Department of Health (MDH) to share immunization information from MIIC with enrolled organizations. Hospitals and long-term care facilities who participated in RespSafe last year may already be familiar with VaxCheck. Organizations not yet enrolled in VaxCheck can do so at VaxCheck Portal. Email Health.VaxCheck@state.mn.us with questions.
MIIC public inquiry
Organizations who need a more complete immunization history can direct their employees to access their MIIC immunization record through Docket® or by requesting a copy of their record from MDH. Employees can learn more at Find My Immunization Record.
With the increase in immunization data that MIIC sees during respiratory illness season, we would like to remind providers to use good data quality practices.
- Ensure that you are using the most up-to-date codes and trade names for Influenza, RSV, and COVID-19 vaccines. For more information visit CDC: Fall Season Respiratory Vaccine Codes.
- Gather and send complete demographic data (including client address and phone number).
- When searching for a client in MIIC, ensure that you have clicked manage client to start a new search and are not inadvertently editing an existing client record.
This will help limit the number of accidentally merged clients and provide more complete and accurate immunization and client data in MIIC for your use. Complete immunization records also benefit the public, who are more likely to access these records, rather than contacting providers.
|
|
The problem
A bad merge occurs when two or more clients’ demographic and/or immunization information are accidentally combined together. This can occur through manual merging and automatic data exchange and typically happens when clients have very similar demographic information (e.g., unrelated clients that have the same name and DOB or twins have very similar names).
The MIIC team regularly reviews potential duplicate clients in MIIC, only merging when a minimum of name, birthdate, and one other piece of demographic information matches. Existing records are merged through data exchange when incoming data has a high enough match score. These processes are necessary to prevent duplicate client and immunizations records, and they emphasize the importance of sending complete demographic data for all of your clients. Common names and birthdates pose challenges when trying to determine if two records are the same using automated and manual processes. Without other pieces of demographic information (i.e., middle names, mother’s names, addresses, phones), information could be accidentally combined as there is nothing in MIIC to distinguish them from each other.
The correction
We are notified about potential bad merges through a variety of outlets, including internal review, emails from providers through the Help Desk, or directly from the public when people discover immunizations not belonging to them on a MIIC record they’ve received or accessed. When a bad merge occurs, it takes a lot of coordination between MIIC operations staff, the person that notified us of the bad merge, and the provider(s) that own the immunizations on the MIIC record in question. Un-merging a MIIC record requires manual verification of all demographic and immunization information and then manually correct the records.
While MIIC operations staff do the manual un-merging of records in MIIC, we rely on the providers that submitted the immunizations on these records to confirm which client they actually gave or entered immunizations for, as we do not have access to anything other than the currently combined record. MIIC staff will reach out to each of the providers that own immunizations on this record, requesting they verify which clients they have seen as well as any demographics or immunizations they know belong to their client. When everything has been verified, MIIC staff will manually create new MIIC records, delete and re-add immunizations to the appropriate records, and update the client information on each record to reflect only their own verified information.
This process can take an inexact amount of time to complete, depending on the specific record and how long it takes to get a response from all of the providers in the verification step. The longer it takes to correct these bad merges in MIIC, the more likely it is for information to continue to be added to the wrong record(s), and the more likely these bad merges are to be queried and reconciled into provider EHRs, leading to mixed up records within your own system. When bad merges are discovered through processing public inquiry requests, clients also have to wait on these corrections before receiving their MIIC immunization records, which they may need for school or child care enrollment, or work.
What can you do?
There are a few things you as providers can do to both prevent bad merges in MIIC and make sure they are cleaned up quickly when found:
-
Always enter/send complete and current demographic data for your clients. This gives our merging processes more information to distinguish clients from each other and helps prevent those who truly have the same or very similar names and birth dates from being accidentally merged.
-
Be careful when searching or updating clients in MIIC. Do not type over client information, rather than starting a new search, to create a bad AKA. Also ensure that you verify all information on a MIIC record matches your patient before updating anything in MIIC or reconciling their MIIC record into your EHR.
-
Respond quickly when MIIC staff reaches out for verification when bad merges occur. We cannot correct these records without your help and the sooner we hear back from you, the sooner we can correct the issue and provide accurate information to both you and the client.
Every year MIIC assessment reports (child, adolescent, and single vaccine/flu) undergo minor changes to update the statewide immunization rate data. Assessment reports were updated in August to reflect data as of July. All users using these reports should now see the updated averages as well as updates to their related footnotes.
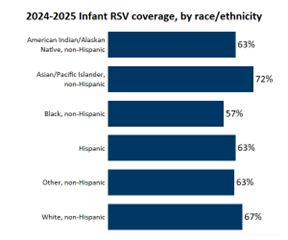
During the 2024-25 respiratory illness season, we had our first opportunity to calculate RSV protection among infants. Nirsevimab shortages in previous seasons made it difficult to interpret this data. Our analysis focused on Minnesota born children entering their first RSV season (birthdate range: 4/1/2024-3/31/2025). RSV coverage was defined as either the birthing parent receiving Abrysvo at least 14 days prior to birth or the infant receiving nirsevimab after birth.
Overall, 57% of MN-born children entering their first RSV season were protected against RSV. Coverage varied by race/ethnicity. Asian/Pacific Islander, non-Hispanic infants had the highest rates (72%). Black, non-Hispanic infants had the lowest rates (57%).
 |
|
As we enter another respiratory illness season it is important to remember that there are two options to protect infants from RSV. By vaccination during pregnancy or through infant immunization. For more information on the options available visit Pregnancy and Vaccination or Vaccines for Adults. |
|
|
|
The following interview has been edited for clarity and length.
Name(s) and position(s)
Sara Meemken, Director of Pharmacy and Ted Simper, Pediatric Pharmacist.
What did CentraCare’s planning process look like when preparing for nirsevimab administration in a birthing hospital setting?
Our journey towards offering nirsevimab to all qualifying infants born in our facility and in the NICU started when Ted Simper, Pediatric Pharmacist at our facility, gave a lecture on pediatric infectious diseases including RSV at the Minnesota Society of Health System Pharmacists annual meeting the spring prior to nirsevimab coming on the market. His talk caught the attention of the representative and medical science liaison from Sanofi, and they met several times to review the data, pharmacology, and pharmacokinetics of nirsevimab. He was impressed by the data which showed a significant decrease in RSV hospitalizations and brought this data forward to pharmacy and pediatrics leadership. The medication received approval through the facility P&T committee and, given compelling data, it was decided to put patients first and offer the vaccine while understanding the hospital in many cases would not be reimbursed for the cost.
Can you tell us about the coordination that occurs to verify the birthing parent’s RSV vaccination status?
We worked with the Epic EMR team to create an ordering panel to help the providers assess which infants qualify for nirsevimab. The infant does not qualify for nirsevimab if the birth parent received Abrysvo RSV vaccine greater than 14 days prior to delivery because they will be protected with mom’s RSV antibodies. The panel asks the ordering provider “Did mom receive the RSV vaccine during pregnancy greater than 14 days prior to delivery?” If the answer is yes, the order states, “Patient does not require nirsevimab (Beyfortus)” and does not allow the provider to order nirsevimab. If the provider answers no, then it asks if the patient is less than 5 kg to allow them to order nirsevimab 50 mg dose or the 100 mg dose for the patients 5 kg or greater. In the NICU, the pediatric pharmacist will also verify the birth parent’s vaccination status.
What other challenges has St Cloud Hospital faced in administering nirsevimab to newborns?
The first year we had the challenge of a supply shortage and determining which patients would receive nirsevimab. Sanofi altered how they provided the immunization this past year, however, and we had a stable supply. We are currently in the process of becoming enrolled in MnVFC using the replacement method, as the separate stock method would have been challenging as an inpatient facility. As one of the first birthing hospitals pursuing this program, we are navigating new terrains in terms of report builds, etc. A final challenge is parents refusing the maternal RSV vaccine and the infant [product] nirsevimab, along with overall vaccine hesitancy.
Share a success you’ve seen since beginning nirsevimab administration in the birthing hospital.
So far, we have administered 551 doses of nirsevimab to infants at the hospital, with 448 in the birth center, 90 in the NICU, and 13 on the pediatric unit. The success of administering nirsevimab to this number of patients prior to discharge was demonstrated in the low number of patients who were hospitalized with RSV throughout the season. None of the pediatric patients that were hospitalized for RSV bronchiolitis had received nirsevimab. With two of the patients, the mom received the RSV vaccine during pregnancy. This is a success to see fewer infants requiring hospitalization for RSV.
What advice do you have for other hospitals considering RSV-mab administration for newborns?
Our first recommendation is to do it. Pediatric providers and pharmacists have been waiting years for an effective immunization against RSV and now we have a great option. The MnVFC program is a great way to recover costs associated with providing this protection to a vulnerable patient population. The application process can appear daunting, but you have a lot of support along the way. Work with your billing team to optimize reimbursement among different commercial insurance payers, and work with your EMR team to build panels to more easily determine which infants qualify for the vaccine.
What other immunization projects are you/your organization planning/looking forward to?
We are looking forward to becoming one of the first MnVFC birthing hospital sites in the state. At the same time, we are now navigating concerns relating to immunization recommendations from ACIP and the CDC. At this time, we continue to follow AAP immunization guidelines for pediatric patients.
|
|
|
|
|
