CLINICAL GUIDANCE
Last year, our partners at the University of Minnesota published part of their report titled, Trauma-informed care and screening for stress and emotional disorders in Afghan refugee children in Minnesota Medicine: July/August 2024 (pages 32-34).
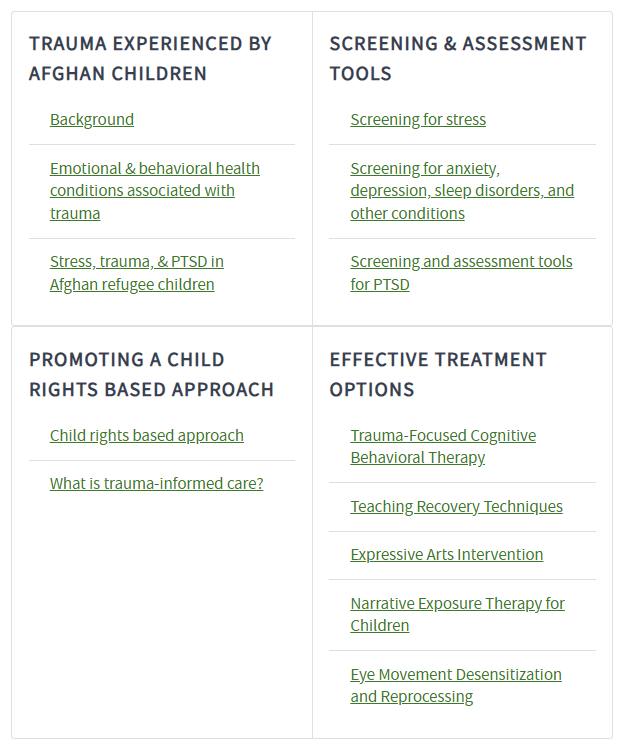
The MN COE has now published the report in full online: Trauma-informed Care, Tools, and Treatment Strategies for Afghan Refugee Children.
We have added the resource to our Afghan Clinical Guidance collection. This comprehensive report covers the trauma experience of Afghan refugee children, promoting a child rights-based approach, trauma screening and assessment tools (available in English, Dari, and Pashto), and effective treatment options.

We reached out to our COE subject matter expert, Dr. Janine Young, to gain some insight into the issue of oral health.
Dr. Young is a professor of Academic General Pediatrics at the University of California – San Diego (UCSD) Department of Pediatrics and is the division chief of Academic General Pediatrics, Newborn Medicine and Developmental-Behavioral Pediatrics. She is the Martin T. Stein Endowed Chair of Developmental Behavioral Pediatrics and holds a joint position within the UCSD School of Public Health. She teaches and mentors medical students, residents, and fellows. Dr. Young is the MN COE principal investigator for UCSD.
|
Why is screening for oral health in newcomers an important component of the domestic medical exam (DME)?
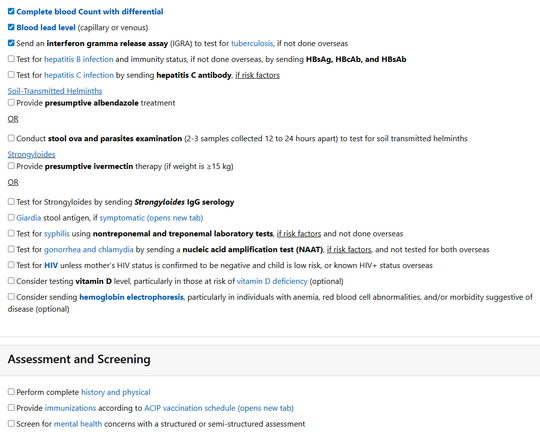
Oral health screening for newcomers is an essential component of the DME: CDC: History and Physical | Refugee Health Domestic Guidance. Many newcomers have never had access to any dental care, including preventative care. They may have untreated caries (cavities), dental abscesses, signs and symptoms of micronutrient deficiencies (e.g., glossitis, perioral dermatitis), and undiagnosed oral-pharyngeal cancers. Infants and young children may have unrecognized oral pain due to untreated caries that can lead to decreased desire or ability to eat food; this can lead to poor weight gain. In these cases, newcomers need to be linked to urgent dental evaluations and treatment.
How can primary care support oral health?
The primary care team can use clinical visits to educate children and adults on proper oral hygiene, including brushing and flossing twice daily. For infants and children who may not yet be able to brush their own teeth, encourage parents to help their children and to use a pea-sized amount of toothpaste for any young children who may swallow the toothpaste. Additionally, pediatricians are encouraged to use well-child visits as an opportunity to apply fluoride varnish to the teeth of infants and young children with primary teeth in accordance with their state’s guidelines. Studies like The Role of Fluoride on Caries Prevention show that two or more applications of fluoride per year decrease the prevalence of dental caries by upwards of 30%. Fluorinated tap water is essential for caries prevention – educate families on the benefits of drinking tap water over bottled water.
What type of oral health patient education should be prioritized during the DME?
Newcomers come with a varied history of health access, so it is crucial to evaluate each individual and family for oral health practices and knowledge. Primary care providers should recommend or directly refer their patients from age 1 year and older to a dentist and encourage families to have preventative care visits with a dentist every six months. Some families may benefit from educational conversations around certain practices that may increase the risk for infection transmission (including sharing oral flora that cause cavities, hepatitis B, C, and/or HIV), or dental caries, including:
- Not sharing toothbrushes.
- Preparing pureed foods by mashing them with a fork, and not by pre-chewing food.
- Explaining how to brush teeth, and potentially showing a toothbrush and toothpaste to families who are unfamiliar with or have not previously owned these items.
- Describing the importance of caring for children’s teeth, even though they will be replaced by adult teeth.
- Emphasizing that everyone should use fluoride toothpaste, including infants and young children.
- Explaining that untreated caries, pain, and infections, even in children’s teeth, can lead to serious health issues, including dental abscesses, other serious infections, and weight loss in children.
How can oral health affect successful resettlement to the U.S.?
- Appropriate referral and linkage to ongoing dental care is essential for newcomer children and adults to treat caries, decrease pain, screen for oral pharyngeal cancer, and to allow for education about appropriate dental care and ongoing preventative visits.
Oral health resources:
- For clinicians:
CDC: Domestic Refugee Screening Guidance: Oral Health
- For newcomers:
The MN COE Newcomer Education for Wellness (NEW) video series includes an oral health educational video offered in 11 languages.
- Recent oral health publications
- Farokhi, M. R., Muck, A. E., Nathan, H., Yan, J., Estacio, A., Su, R., Stone, M., Mandlik, N., & Worabo, H. (2025). Harnessing technology to enhance oral health literacy among Afghan women: an interprofessional community-engaged initiative. Frontiers in public health, 13, 1594767. doi:10.3389/fpubh.2025.1594767
- Kandahari, N., Moulana Zada, F., & Farzal, Z. (2025). The Oral Health Disparity Among Refugee Children: A Systematic Review. Laryngoscope investigative otolaryngology, 10(4), e70194. doi:10.1002/lio2.70194
TRAINING OPPORTUNITIES
The following recorded webinar is now available on our Trainings webpage:
Recordings available soon:
- Considerations for Nutrition and Growth in Newcomer Families
- From Arrival to Aisles: Pharmacy Support for Newcomers
PUBLICATIONS
The Migration Health Initiative (MHI) at the Task Force for Global Health created the Hepatitis B Dialogue Guide to provide health care providers with the information and support needed to make informed decisions about hepatitis B screening and vaccination when they counsel refugee, immigrant, and migrant patients.
Designed with a human-centered approach, the guide includes four key concepts:
-
Starting the conversation: principles and strategies to build trust in a culturally attuned way, covering topics like stigma, family dynamics, and patient voice.
-
Establishing the facts: simple, visual cards to guide the conversation, address misconceptions, and build trust.
-
Exploring mindsets: strategies to help providers understand - and respond to - patient perspectives and beliefs in a respectful way.
-
Planning next steps: pathways to develop next steps with the patient.
Take a moment and review some recent publications on newcomer health:
- Connor, J. J., Abdi, C., Chen, M., Salad, M., Pergament, S., Afey, F., Hussein, I., & Robinson, B. B. E. (2025). Our Body Our Health (Jirkeena, Caafimaadkeena): Somali Women's Narratives on Sexual Health. Journal of sex research, 62(7), 1253–1267. doi:10.1080/00224499.2023.2288077
- Smith, D. C., Thumm, E. B., Tien, N. C. G., & Kissler, K. (2025). Respectful maternity care experiences of South Asian refugees in the US: a qualitative study. Frontiers in public health, 13, 1613249. doi:10.3389/fpubh.2025.1613249
- Virk, S. K., Tham, S., Hatef, C., Oren, T., Berger, L., Tucker, A., Milewski, A. R., de Melo-Martin, I., & Kaur, G. (2025). Acceptability and Barriers to Chronic Pain Treatment in Refugee Torture Survivors. JAMA network open, 8(8), e2529775. doi:10.1001/jamanetworkopen.2025.29775
- Nassur, J., Dajee, D., Leader, A., & DiSantis, K. (2025). Barriers to Breast, Cervical, and Colorectal Cancer Screenings Faced by Refugees Resettled in the United States: A Rapid Review. Journal of immigrant and minority health, 27(4), 609–622. doi:10.1007/s10903-025-01690-1
- Connolly, S., Liebermann, E., Greaney, M. L., Cohen, S. A., Lindsey, H., Prue, O., & Keller, J. C. (2025). "They were saying that it's the end of the world": Experiences of COVID-19 and beliefs about the COVID-19 vaccine among refugees in Rhode Island, US. Human vaccines & immunotherapeutics, 21(1), 2550097. doi:10.1080/21645515.2025.2550097
|