|
Telehealth1 may be one of the few silver linings of the COVID-19 pandemic. Although some health professionals were reaching their patients via dedicated computer platforms before COVID, it was still a relatively uncommon practice. Things have changed. In this Spotlight we compare the use of telehealth in 2022 to 2019. These two time periods present the year right before the arrival of COVID and a time period two years into the pandemic. Changes between the two periods can be loosely interpreted as the “COVID effect.” In general, the data suggests that telehealth—an occasional practice before COVID—is now a firmly-rooted and widespread mode of care in specific professions, settings, and regions. Unless otherwise stated, the data presented here comes from the Minnesota Healthcare Workforce survey collected from two periods in time: (1) calendar year 2019; and (2) October, 2021 through July 2022 (for ease, this second period is labeled “2022” in the charts below).
Changes in telehealth use
We begin by looking at telehealth use across eight professions. Figure 1 shows the percentage of clinicians who report having used telehealth for at least some of their patient/client encounters in 2019 compared to 2022.2 The change varies by profession. However, in all but two professions (respiratory therapists and registered nurses) the share of providers who now use telehealth has increased considerably. Among mental health providers, for example, the share of clinicians using telehealth has nearly quadrupled. Likewise, the share of physicians using telehealth more than doubled, in what is sure to reflect a major change in clinic operations and patient care. As noted, the registered nurse and respiratory therapist findings run counter to other professions, a finding which we discuss below.
Figure 1: Share of clinicians who report using telehealth to treat patients or
clients at least some of the time, BY PROFESSION, 2019 AND 2022

Figure 2 shows telehealth use across different work settings. Here we see that in some settings—notably clinics and professional offices, postsecondary institutions, public health agencies, and community/faith-based organizations, more than double the share of providers report using telehealth in 2022 versus 2019. But again, there is unevenness: telehealth has decreased in several settings, including home health care, hospitals, and long-term care.
Figure 2: Share of clinicians who report using telehealth to treat patients or
clients at least some of the time, BY SETTING, 2019 AND 2022

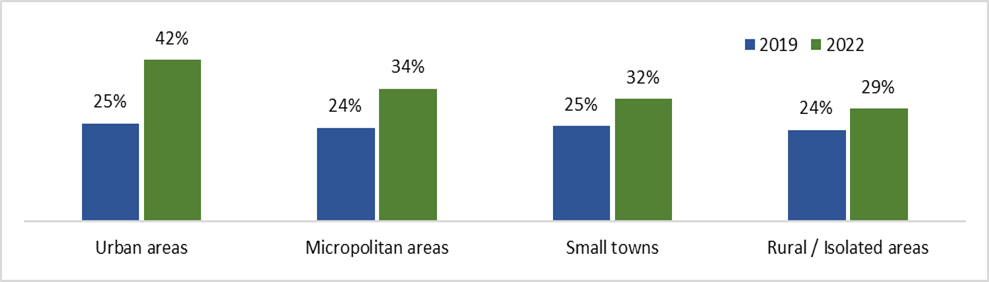
Finally, we compare urban and rural areas in the movement toward telehealth (see Figure 3). As we can see, the biggest change happened in large metropolitan areas, where the percentage of providers using telehealth grew modestly from 25 to 42. The more rural the area, the less adoption of telehealth.
Figure 3: Share of clinicians who report using telehealth to treat patients or
clients at least some of the time, BY REGION OF MINNESOTA, 2019 AND 2022
The findings presented here show that telehealth use has grown quickly throughout the pandemic, but that the expansion has not been universal. Rather, it has been concentrated in certain occupations, work settings, and regions, with some sectors and occupations actually showing a decline in telehealth use. Mental health and substance use disorder counselors, physicians, and physician assistants all increasingly adopted telehealth as a mode of patient care, whereas registered nurses and respiratory therapists were actually less likely to use telehealth than they were before COVID. Likewise, telehealth use increased dramatically in clinics, postsecondary academic institutions, public health agencies, and community/faith-based organizations, but declined in hospitals. And finally, telehealth use expanded in heavily urban areas of the state and far less dramatically in rural areas.
What might be causing these patterns?
The data presented here cannot speak to the underlying causes of these differences, but we can make some educated guesses. It could be that registered nurses and respiratory therapists, who tend to work in acute care settings such as hospitals, are treating more patients with conditions that are not appropriate for remote consultation or care than they were in 2019.
Regarding the regional differences, we might speculate that the lack of reliable internet constrains the adoption of telehealth. We might also speculate that rural providers being, on average, older than their urban counterparts were perhaps less embracing of technology for health care use. However, an analysis of telehealth adoption by age (not shown in this brief) does not support this argument: older clinicians are no less likely than younger ones to have moved toward telehealth between 2019 and 2020. Certainly, being able to communicate with patients in this way has great potential to increase access to patients who live in remote and frontier areas of the state, so rural clinicians might be even more motivated to use telehealth than those in urban areas.
This begs the question: does telehealth indeed expand health care access to rural communities? This is a common claim, and additional survey data shows there is strong evidence that it does. Clinicians who use telehealth report that they regularly provide care to those who are located in areas that are more rural than where they practice (see Figure 4). In fact, more than a quarter of providers who use telehealth report that they are providing care to people in more rural areas on at least a daily or weekly basis. Moreover, an additional analysis not included in this article indicates that this result does not change when disaggregated by region; the finding holds true for providers in both urban and rural areas.
Figure 4: Responses to the question: “Not including those who are on vacation
or at a cabin, how often do you provide care via telemedicine to people who live
in areas that are more rural than where you practice?” (All providers who report
using telehealth, 2022)

The findings presented here indicate that although adoption of telehealth is concentrated among certain providers in certain settings, it has clearly grown as a regular mode of practice in those sectors. Telehealth is here to stay, and it has great potential to expand access to rural communities who face barriers in accessing care.
Endnotes
1 We are using the term “telehealth” rather than “telemedicine” here to reflect the fact that this mode of care is used in both medical settings (such as physicians’ offices) and settings that are not typically considered medical, such as mental health or substance use treatment facilities.
2 Note that this is not a measure of how often telehealth is being used, but how many clinicians are using telehealth. The count includes those providers who use telehealth only very occasionally, to providers who use telehealth exclusively.
About the Health Workforce Analysis program
The Health Workforce Analysis program is housed within the Office of Rural Health and Primary Care. Research staff collect and analyze Minnesota-specific data on nearly 20 different licensed health care professions to understand the availability, distribution and demographics of the workforce. The data are used to inform healthcare workforce policies and investments.
|


