|
View this as a webpage
September 2022
Pregnancy Risk Assessment Monitoring System (PRAMS) is a surveillance project conducted by Centers for Disease Control and Prevention’s (CDC) Division of Reproductive Health in collaboration with the Minnesota Department of Health (MDH). The PRAMS survey asks new moms about maternal behaviors, attitudes, and experiences before, during, and shortly after their pregnancies. Participants are resident women who recently gave birth in Minnesota to a live-born infant during the surveillance year. Women are sampled between 2 and 6 months after giving birth.
First-ever Minnesota Maternal Mortality Report Reveals Opportunities to Prevent Maternal Deaths
The Minnesota Department of Health’s Maternal Mortality Review Committee (MMRC) reviewed 48 pregnancy-associated deaths in Minnesota that occurred during 2017-2018. Pregnancy-associated death is a death that occurs during pregnancy or within one year of termination of pregnancy irrespective of cause. The findings of the review committee and recommendations can be found in Minnesota’s first Maternal Mortality Report. This report also includes demographic information and characteristics of pregnancy- associated deaths of Minnesotans, summarizes the causes of deaths, and factors contributing to these deaths.
PRAMS Highlights
We are excited to announce that Minnesota PRAMS (MN PRAMS) met the minimum response rate threshold for 2020!
MN PRAMS was recently selected and awarded funding by the Council of State and Territorial Epidemiologists (CSTE) to implement a Social Determinants of Health (SDOH) supplemental questionnaire from May 2022 through March 2023. SDOH factors like food insecurity, housing, access to health care, social support, transportation barriers, and racism can have a major impact on the immediate and long‐term health of pregnant and recently postpartum women and their infants,1 so we are happy to be given the opportunity to collect data on this important topic.
MN PRAMS currently offers two modes of data collection- mail and phone. However, testing is underway for the Web Survey Module (WSM) that will allow participants to complete our survey on the web. Minnesota was selected as one of ten states to carry out phase 1 testing of the WSM. The web survey is expected to be implemented in Fall 2022.
The Phase 9 question selection process is still underway. PRAMS sites received a list of 160 prospective questions for Phase 9 Core and each state voted on questions to keep, drop, or add to Phase 9 Core. CDC has sent the final Phase 9 Core and Standard question lists to PRAMS sites. We will be working with partners and our advisory committee to identify gaps, identify priority areas, and select a prioritized list of standard and site-specific questions for the Phase 9 survey.
The MN PRAMS Advisory Committee is required by the CDC, to advise the Minnesota PRAMS staff in the development and selection of state-specific questions and on the use, dissemination, and application of findings. The multi-disciplinary committee includes individuals from the public, private, and academic sector (city, county, state, and tribal agencies; academic centers; health plans and medical centers; and maternal child health nonprofit organizations). MN PRAMS is recruiting Maternal and Child Health (MCH) experts who are interested in joining our advisory committee. In our efforts to increase diverse voices to the advisory committee, we are also looking for community organization representatives for American Indian families, and representation from Greater Minnesota. If interested, contact us at: HEALTH.MNPRAMS@state.mn.us
Black Maternal Health
This quarter’s newsletter aims to bring awareness to Black maternal health, highlight health outcomes using MN PRAMS data, and prompt action to reduce disparities and poor health outcomes among Black women.
- The U.S. has one of the highest rates of maternal mortality among high-income countries and rates have been increasing.2
- Black women are three times more likely to die from a pregnancy-related cause than white women.3
- In Minnesota, preliminary data from 2011-2017 show that the maternal mortality rate for non-Hispanic Black women is 2.3 times higher when compared to white mothers. The American Indian maternal mortality rate is approximately 4 times higher than that for white mothers.4
- Social determinants of health (access to care, income, housing, education, neighborhood, etc.)- the conditions which affect health and quality of life outcomes- play a role in these disparities.
- Systemic racism experienced by Black communities for the past 400 years underlies many aspects of social determinants of health and continues to influence policies and practices, leading to poor outcomes in Black maternal health today.
Chronic Conditions
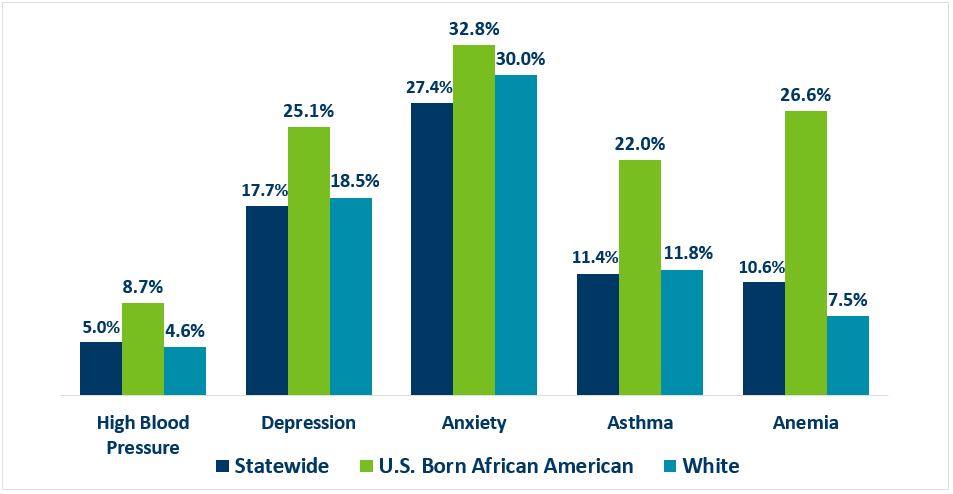
Chronic conditions that increase the risk of adverse health outcomes for moms and their newborns are increasingly prevalent among childbearing women.5 As the number of different chronic health conditions goes up, so does the risk of severe maternal morbidity and mortality.6 Figure 1 shows the percentage of women who reported high blood pressure, depression, anxiety, asthma, and anemia three months before pregnancy. For all five conditions shown, U.S. born Black women reported percentages that were higher than the statewide prevalence. The biggest disparities are seen for depression, asthma, and anemia. About 25% of U.S. born Black women reported depression three months before pregnancy compared to roughly 18% of all women in Minnesota. Percentages of Black women with asthma three months before pregnancy were almost twice that of all Minnesota women (22.0% vs 11.4% respectively) and percentages of Black women with anemia three months before pregnancy were more than two times that of all women in Minnesota (26.6% vs 10.6% respectively).
Figure 1- Self-Reported Health Conditions 3 Months Before Pregnancy, PRAMS 2016-2020
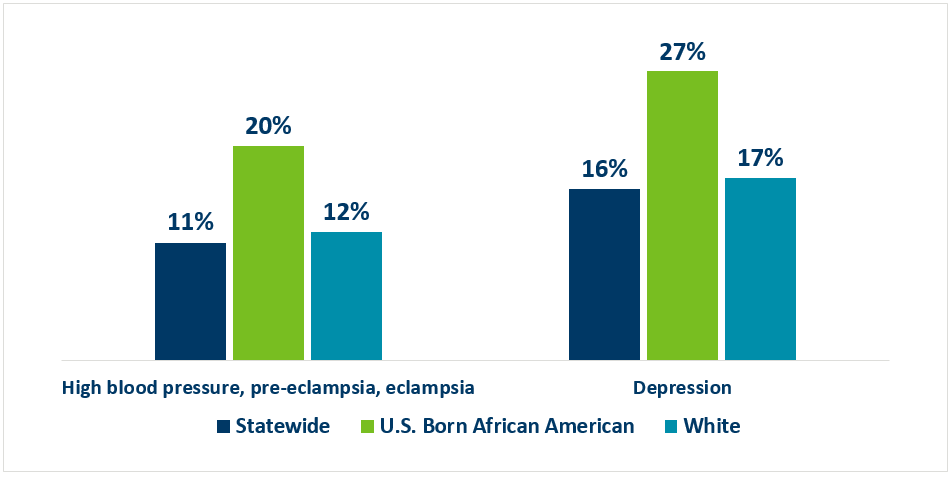
MN PRAMS data also showed that U.S. born Black women are also more likely to have self-reported chronic conditions during pregnancy. Figure 2 shows that 20% of U.S. born Black women said they had high blood pressure (that started during their most recent pregnancy), pre-eclampsia, or eclampsia. This percentage was almost two times the statewide prevalence. Additionally, 27% of U.S. born Black women reported having depression and this was also higher than the overall percentage (16%).
Figure 2- Self-Reported Health Conditions During Most Recent Pregnancy, PRAMS 2016-2020
 Barriers
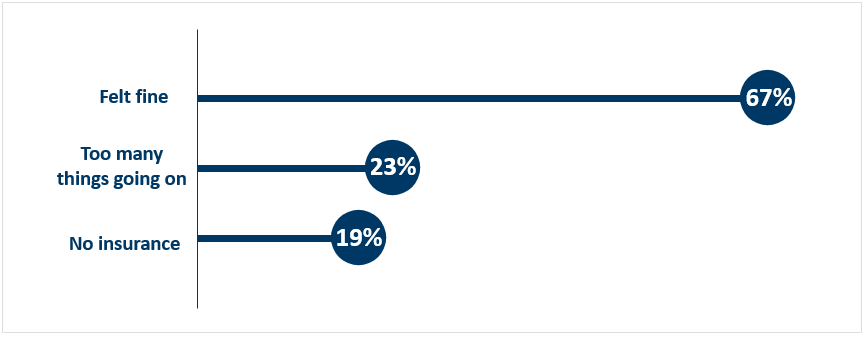
Access to health care visits before pregnancy can allow for early diagnosis and treatment of preexisting chronic conditions like high blood pressure or anemia which if not appropriately addressed, can cause severe complications or death during and after pregnancy. U.S. Born Black women who did not have any health care visits 12 months before they got pregnant identified barriers to obtaining preconception care. The top three barriers are shown in Figure 3. In Minnesota, 67% of U.S. born Black women did not attend any health care visits 12 months before they got pregnant, because they felt fine and did not feel they needed to have a visit. This was the biggest barrier identified. Having too many things going on (23%) was identified as another barrier, followed by not having health insurance to cover the cost of the visit (19%). Some barriers such as having no insurance are structural or systemic and can be modified to improve accessibility.
Figure 3- Top 3 Barriers to Preconception Care Among U.S. Born Black Women, PRAMS 2016-2020
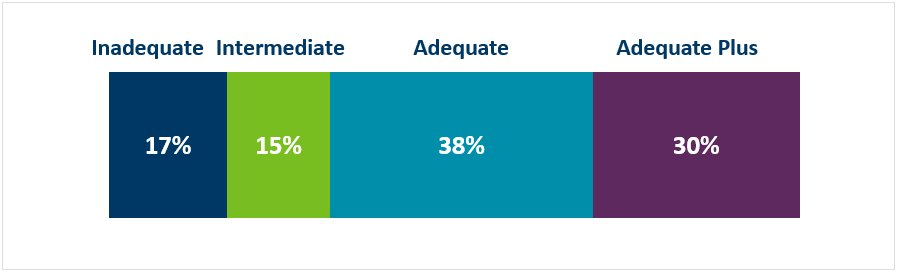
Prenatal care is essential for optimal health of mothers and babies throughout pregnancy and delivery. Figure 4 shows that nearly one in three births were to U.S. born Black women who had less than adequate (includes inadequate and intermediate responses) prenatal care as determined by the Adequacy of Prenatal Care Utilization Index (Kotelchuck). The index defines inadequate prenatal care as having less than 50% of the expected prenatal care visits and intermediate prenatal care as 50-79% of the expected prenatal care visits.
Figure 4- Adequacy of Prenatal Care Among U.S. Born African American Women, PRAMS 2016-2020
As a result of systemic racism, U.S. born Black women face barriers that prevent them from accessing early, adequate, and quality prenatal care:
Healthcare Experiences
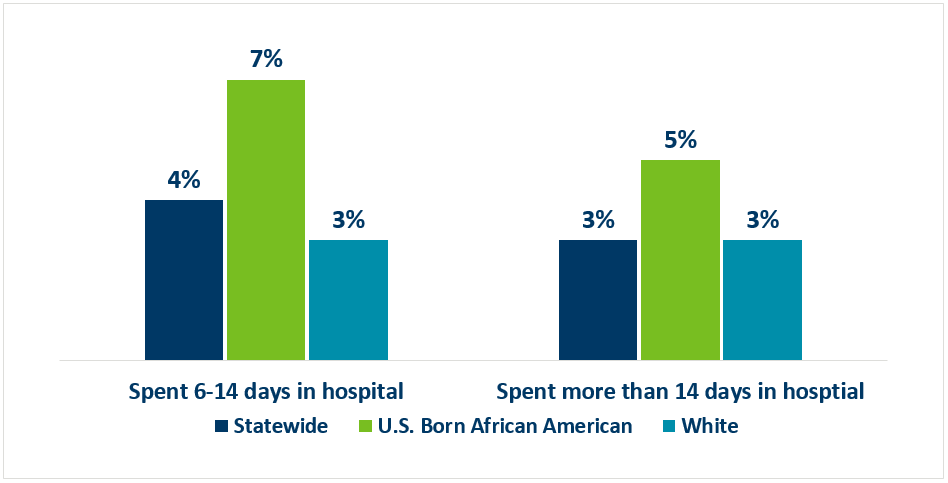
Our data also revealed disparities among U.S. born Black women with respect to birth outcomes, specifically the length of stay of their babies after delivery. Figure 5 shows that 7% of U.S. born Black women reported their babies spent 6-14 days in the hospital after delivery compared to 4% of all Minnesota women. Furthermore, 5% of U.S. born Black women said their babies spent more than 14 days in the hospital after delivery compared to 3% of women in Minnesota.
Figure 5- Self-Reported Baby Length of Stay After Delivery, PRAMS 2016-2020
Experiences with Racial Discrimination
Below are comments from U.S. born African American women who responded to our survey:
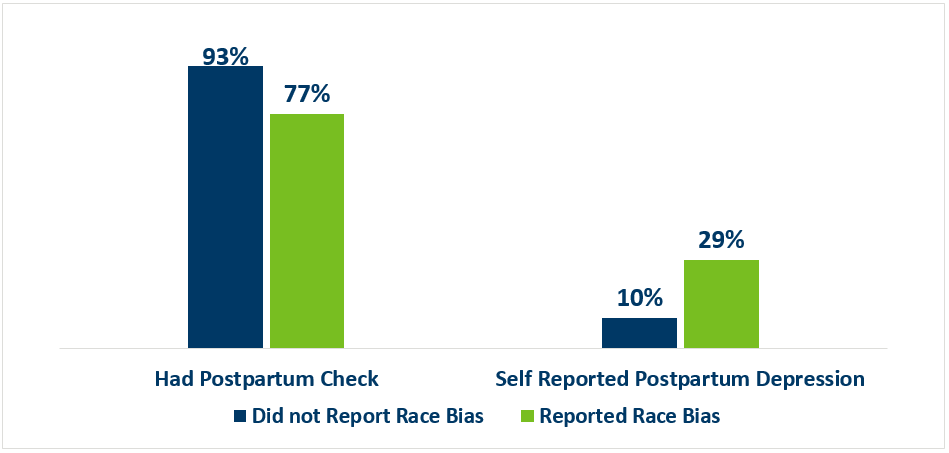
The MN PRAMS survey asked the following question- ‘During the 12 months before your baby was born, did you feel emotionally upset (for example, angry, sad, or frustrated), as a result of how you were treated based on your race?’. We found that women who responded yes to this question were less likely to have a postpartum checkup and more likely to self-report postpartum depression. As Figure 6 shows, 77% of women who felt emotionally upset due to the way they were treated because of their race, reported they had a postpartum checkup compared to 93% who did not report being treated badly because of their race. In addition, women who reported feeling emotionally upset before pregnancy as a result of how they were treated based on their race were almost three time more likely to self-report postpartum depression compared to women who did not report being treated badly based on race (29% vs 10% respectively).
Figure 6- Postpartum Check Up and Self-Reported Postpartum Depression Among Women Experiencing Racial Bias Before Pregnancy, PRAMS 2016-2020
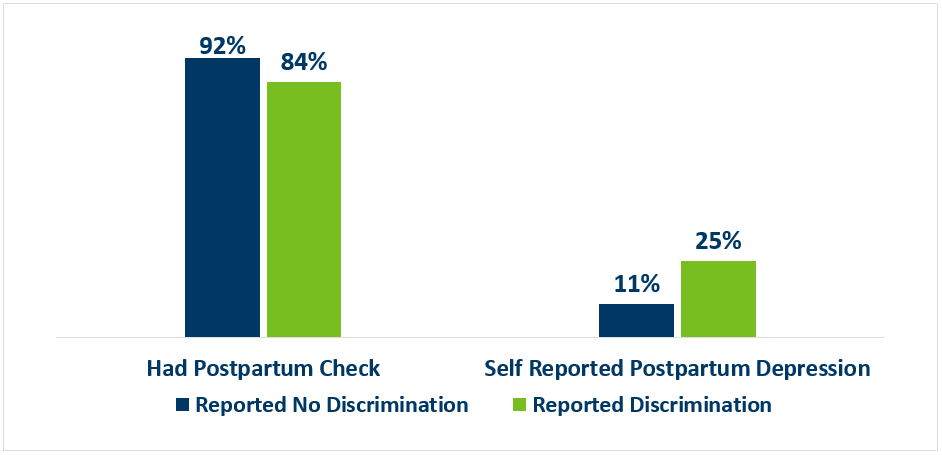
MN PRAMS data also shows that women who experienced discrimination by health care providers during their prenatal care, labor, or delivery because of their race, ethnicity, or culture were less likely to have a postpartum checkup and were over two times more likely to self-report postpartum depression compared to women who did not report discrimination. As shown in Figure 7, 84% of women who said they experienced discrimination by health care providers during their prenatal care, labor, or delivery because of their race, ethnicity, or culture, had a postpartum checkup for themselves compared to 92% of women who did not report discrimination. Additionally, 25% of women who experienced discrimination by health care providers based on their race, ethnicity, or culture during prenatal care, labor, or delivery self-reported postpartum depression compared to 11% who did not report discrimination.
Figure 7- Postpartum Check Up and Self-Reported Postpartum Depression Among Women Experiencing Racial Discrimination by Healthcare Providers During Prenatal Care, Labor, or Delivery PRAMS 2016-2020
- Expand family-focused, community-based policy and funding for women's care before, during, and after pregnancy by:
- Expanding the immediate family’s role in care and the birthing process.
- Ensuring that funding and policy is reflective of the communities they are intended to serve.
- Increase access to paid family leave.
- Integrate health and social services and optimize cross-sector collaboration to benefit women and infants. By integrating existing services, promotion of preventative health becomes an option for pregnant women and babies and allows families to work with a care team.
- Strengthen and expand culturally responsive, trauma-informed care. This will allow pregnant women to have more autonomy while seeking services and will help them build a trusting relationship with their health provider.
- Emphasize the importance of attending health care visits throughout the life course but particularly before conception and in the fourth trimester so that chronic conditions can be identified and treated early.
- Health care providers and systems need to listen more closely to the concerns of their patients. Communication should be enhanced to ensure that women feel heard and informed throughout the birth process.
- Recognize and address implicit bias in healthcare.
- Build and create access to a more diverse healthcare workforce, including midwives and doulas.
- Address social determinants of health factors affecting maternal health, including housing, economic stability, and community support.
- Promote the positive role of fathers, partners and other family or support people in pregnancy and postpartum care.
- https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health
- (OECD, U.S. Census Bureau)
- Centers for Disease Control and Prevention: Working Together to Reduce Black Maternal Mortality
- Minnesota Department of Health: Maternal Mortality
- Centers for Disease Control and Prevention: Pregnancy Mortality Surveillance System
- Centers for Disease Control and Prevention: Obstetric Outcomes and Delivery- Related Healthcare Utilization and Costs Among Pregnant Women with Multiple Conditions
|



