|
View this as a webpage
Winter 2021/2022
Pregnancy Risk Assessment Monitoring System (PRAMS) is a surveillance project conducted by Centers for Disease Control and Prevention’s Division of Reproductive Health in collaboration with the Minnesota Department of Health (MDH). The PRAMS survey asks new moms about maternal behaviors, attitudes, and experiences before, during, and shortly after their pregnancies. Participants are resident women who recently gave birth within Minnesota to a live-born infant during the surveillance year. Women are sampled between 2 and 6 months after giving birth.
PRAMS Highlights
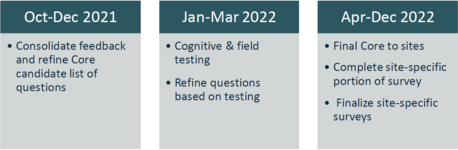
- PRAMS is currently engaged in the phase 9 questionnaire revision process. A timeline for the remaining steps in the process are listed below:
- The web survey module (WSM) implementation began in five early adopter sites (MD, PR, SC, VA, WY) this fall. WSM will be deployed in additional PRAMS sites in phases during 2022.
Safe Sleep
November 14-20, 2021, is Infant Safe Sleep Week in Minnesota! The goal of this issue is to use Minnesota PRAMS data to highlight infant sleep practices and promote safe infant sleep in an effort to reduce preventable infant deaths in Minnesota.
Here are some quick facts:
- Minnesota’s infant mortality rate has historically been lower than the U.S. rate overall. In 2019, the infant mortality rate for Minnesota compared to the US was 4.6 versus 5.6 deaths per 1,000 live births, respectively.1,2
- Despite Minnesota's lower infant mortality rate, there are still significant racial disparities. Recent data show the rates of infant mortality among Black/African American and American Indians were 2.3 and 2.5 times that of non-Hispanic Whites, respectively. 3
-
There are many reasons why babies die in Minnesota. Sudden Unexpected Infant Death (SUID) includes sudden infant death syndrome (SIDS), accidental suffocation and strangulation in bed or other sleeping environments, and deaths from unknown causes. From 2014-2018, SUID was the fourth leading cause of infant mortality in Minnesota.4
-
State health department analysis of the 100 sudden unexpected infant deaths in 2018 and 2019 found that 93% or 93 were sleep-related and happened in unsafe sleep environments, according to preliminary data.5 Thus, the vast majority of SUID in the state are preventable.
A key takeaway for parents and other caregivers is to know the ABCs of safe sleep:
A: Alone. Infant and caregivers can share a room, but not the same sleeping surface. The use of soft bedding (e.g., blankets, pillows, and soft objects) in the infant sleep environment should also be avoided.
B: Back. An infant should be placed to sleep or nap on his or her back.
C: Crib. Place infant on a firm sleep surface such as a mattress in a safety-approved crib or bassinet.
Additional recommendations to reduce the risk for sleep-related infant deaths include having a smoke-free environment, breastfeeding, providing routinely recommended immunizations, and avoiding prenatal and postnatal exposure to alcohol, and illicit drugs.
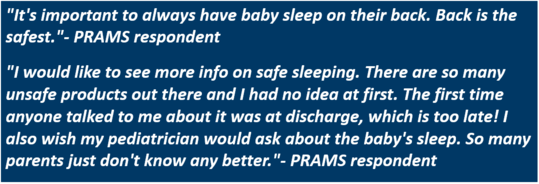
What Minnesota Moms Say About Infant Sleep Practices
Comments from the Minnesota PRAMS survey reveal a need for modeling and teaching infant safe sleep best practices and doing this early on, before hospital discharge:
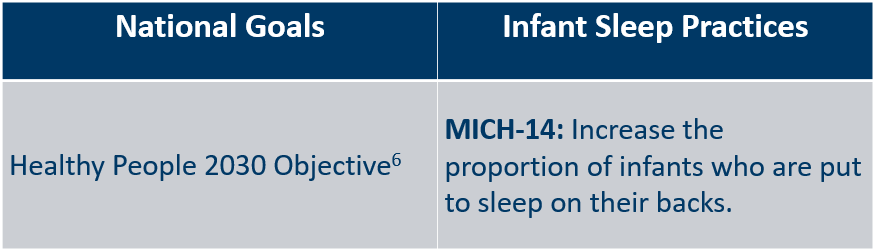
National Goals on Infant Sleep Practices
The Healthy People 2030 Objective on infant safe sleep is tracked using PRAMS data. National Healthy People 2030 guidelines recommend increasing the proportion of infants who are put to sleep on their backs from 78.7% (most recent data available) to 88.9% (MICH‑14).6
Infant Sleep Practices
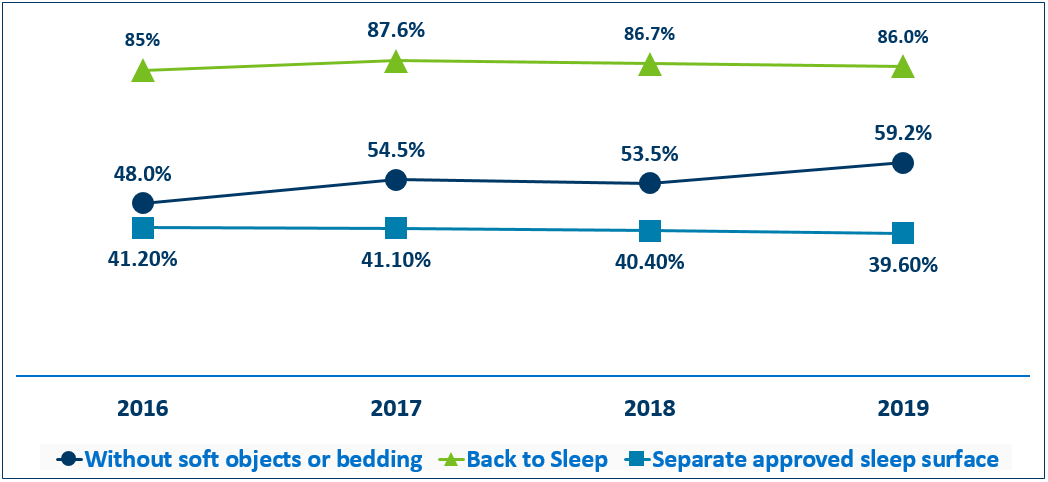
Title V, a source of support for promoting and improving the health and well-being of the nation’s mothers and children, also uses PRAMS data to track outcomes.7 Analysis of Minnesota PRAMS data on infant sleep practices over time (figure 1) shows that the percent of infants placed to sleep on their backs has remained fairly steady from 2016 to 2019. The percent of infants placed to sleep on a separate approved sleep surface declined slightly to 39.6% in 2019. However, the percent of infants placed to sleep without soft objects or loose bedding has increased from 53.5% in 2018 to 59.2% in 2019.
Figure 1- Percent Practicing Safe Sleep Practices Over Time
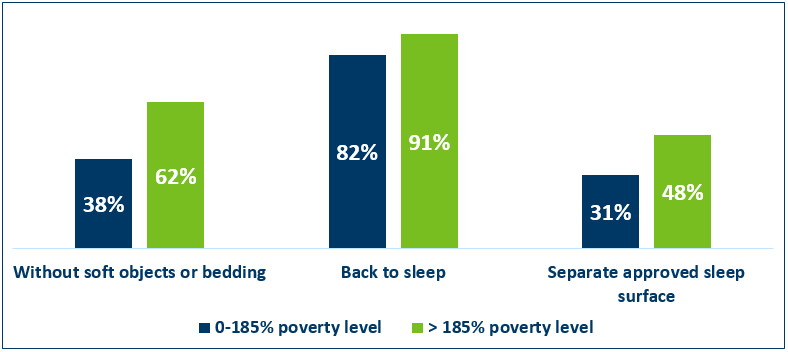
Analysis of combined 2016-2019 Minnesota PRAMS data by Federal Poverty Level (FPL)(figure 2) shows that in Minnesota, low-income respondents (those at or below 185% FPL) practiced infant safe sleep at lower percentages than higher income respondents (those above 185% FPL). Only 38% of low-income PRAMS respondents placed their infants to sleep without soft objects or loose bedding compared to 62% of high-income respondents. Higher percentages of both low- and high- income respondents reported that their infant was placed to sleep on their back. However, 82% of low-income respondents said their infant was placed to sleep on their back compared to 91% of high-income respondents. Even fewer respondents reported placing infants to sleep on a separate approved sleep surface- 31% of low-income respondents compared to 48% of high-income respondents.
Figure 2- Safe Sleep Practices by Federal Poverty Level (FPL) 2016-2019
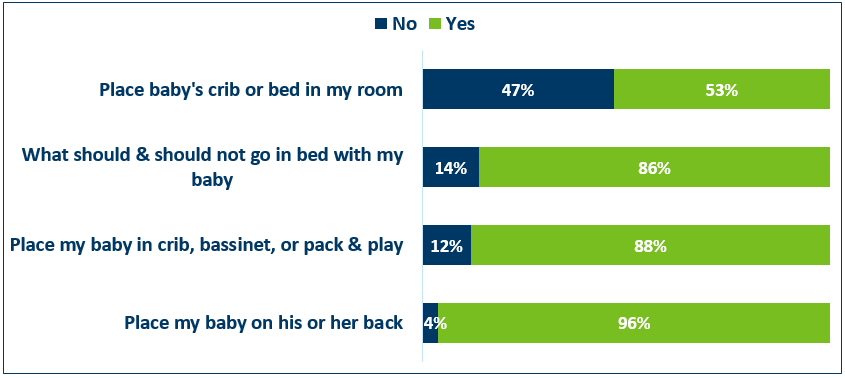
PRAMS respondents were asked the following question by a health care provider: 'Did a doctor, nurse, or other health care worker tell you any of the following things?' Analysis of combined 2016-2019 Minnesota PRAMS data (figure 3) shows that most PRAMS respondents (96%) report that a doctor, nurse, or other health care worker told them to place baby on his or her back. Additionally, 88% of PRAMS respondents say that a doctor, nurse, or other health care worker told them to place infant in a crib, bassinet, or play yard. Similarly, 86% of PRAMS respondents report being told what should and should not go in bed with the baby. About 47% of respondents report not being told by their doctor, nurse, or other health care provider to place the baby's crib or bed in the same room.
Figure 3- Topics Discussed by Doctor, Nurse, or Other Health Care Worker 2016-2019
The following section discusses recommendations and resources:
- To increase awareness and uptake of AAP safe sleep recommendations public health efforts can:
- Improve safe sleep practices in child-care and hospital settings by training providers.
- Use WIC and other programs that serve mothers and babies to deliver culturally appropriate messaging about safe sleep for babies.
- Continue Minnesota initiatives and campaigns around safe sleep education.
- Eliminate inequities to ensure that all babies in our state have an equitable opportunity for a healthy life.
- Healthcare staff should educate parents and other trusted caregivers on infant safe sleep practices during prenatal care visits throughout the course of pregnancy as well as after delivery.
- Hospitals should become safe sleep certified. Hospitals can receive National Safe Sleep Hospital Certification by modeling and teaching infant safe sleep best practices before hospital discharge.
- Continue Minnesota initiatives and campaigns around safe sleep education.
- Continue to provide supports needed to create a safe sleeping environments. One activity the 34 Positive Alternative grantees provide statewide to participants, is portable cribs as well as safe sleep education (link provided under resources).
- Minnesota Center for Health Statistics: 2019 Minnesota Health Statistics Annual Summary
- Centers for Disease Control and Prevention: Infant Mortality
- Minnesota Department of Health: MDH linked birth/infant death file
- Minnesota Department of Health: MDH linked birth/infant death file
-
- Healthy People 2030: Sleep Objectives- Infants
- U. S. Department of Health and Human Services: Guidance Portal
|