|
As our partners know, the refugee health screening contains a range of clinical components. From immunizations to reproductive health and beyond, a successful refugee health screening depends upon clear communication between the health team and the patient. Patients utilized interpreters for 97% (1,773 out of 1,837) of the initial health screenings for people with refugee status arriving between January 1, 2017, and December 31, 2018. This included 29 languages for people from 40 countries.
Communication and language assistance is one of the key areas of the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (The National CLAS Standards). High-quality medical interpretation is both rigorous and full of nuance. Specific words and phrases may not have an equivalent in the target language, and each of us understands health, well-being, and other critical concepts in health care through a cultural lens. Minnesota does not currently have medical interpreter criteria beyond an administrative roster, but many agencies and health systems require training and sometimes certification for their interpreters.
Both providers and interpreters have voiced an interest in training opportunities that address challenging areas of communication with patients who have limited English proficiency. Examples include vaccine hesitancy, family planning, and end-of-life care. Equally important, interpreters and providers expressed interest in an interdisciplinary venue in which each profession could learn from the other. In response to these needs, the Minnesota Department of Health Refugee and International Health Program launched a training workshop series.
With planning committee members from multiple health care systems, subject matter experts, providers, interpreters, and other professionals, the team held two pilot trainings in August 2019. Each training was focused on the topic of interest (for the pilot trainings, the topic was vaccine hesitancy). The training centered on a facilitated interdisciplinary conversation, interweaving considerations of roles, ethical codes, the systemic context, and patient-centered care.
After the successful initial workshops, the team is synthesizing feedback and connecting with potential partners to continue the series. Please reach out to Ellen Frerich (ellen.frerich@state.mn.us) if you are interested in becoming involved in the initiative, would like to host a workshop, or have similar training opportunities to share.

Karissa Studier, a public health nurse with Mower County in southern Minnesota, has been working at the county for nearly six years and in refugee health for approximately three years. Like so many public health nurses, her job duties cover a range of needs and programs. These include visiting with prenatal and postpartum families in their homes as a family home visiting nurse, providing immunizations to those 18 and under with public insurance or no health insurance through the county immunization program, as well as her work in refugee health.
Local public health plays an important role in the health screening offered to newly arriving individuals or families with refugee status. In her role, Karissa reviews overseas health history, communicates with area providers, schedules initial medical and dental assessments, meets with refugee families and provides education, and helps coordinate some follow-up care.
She explains that her favorite part of this work is “learning about the processes that refugee families go through to get resettled somewhere and getting to meet many people from different areas of the world.” In Mower County, residents bring many different languages and cultures. Over 40 languages are represented within the Austin Public School District. See the table below for a summary of refugee arrivals to Mower County in recent years.
|
Mower County Primary Arrivals by Calendar Year and Country/Region of Origin
| |
Burma |
Sub-Saharan Africa* |
Total |
| 2014 |
9 |
1 |
10 |
| 2015 |
15 |
9 |
24 |
| 2016 |
25 |
19 |
44 |
| 2017 |
3 |
1 |
4 |
| 2018 |
21 |
2 |
23 |
*Ethiopia, Eritrea, Sudan
Despite the growing diversity in the area, language access continues to be challenging at times. For some languages that are less commonly spoken, such as Anuak, it can be very difficult to find an interpreter to connect with clients. Another challenge in Karissa’s refugee health work is finding transportation to get clients to and from appointments (which may include specialty care in Rochester).
Karissa and Mower County Public Health are proactive in reaching out to partners. Mayo Clinic Health System-Austin plays a key role in providing health care to much of the community, including refugee health screenings. When the provider doing the majority of refugee health screenings retired last year, a new provider willingly and eagerly stepped in. Joanne McGaffey, CNP, sees nearly every new refugee that comes to Mower County now, and is the first medical provider they encounter in the United States. Through their initial encounter, which usually takes several hours, all the necessary testing and evaluation are completed for the newly arrived refugee families. Interpreters, including the Language Line phone interpretation system, make this work possible for Karissa and for the clinic.
Karissa also acknowledges the critical role played by the case managers at area resettlement agency, Catholic Charities. She reflects, “Catholic Charities are a big connection point for us at Public Health, and we are in communication about family/individual needs required for their medical care. They are in consistent contact with families for their first 90 days in the United States and connect them with so many beneficial resources during that short time frame.”
Karissa sees the impact of the work that she and others do to support new families and welcome them to the community. Her goals are to “begin to establish a new relationship for each refugee and their medical provider” and to “improve overall health in each of these families by educating on who, when, and where to go for care.”
The role of the Refugee and International Health Program at MDH is to support this process across the state in ways that are helpful to our partners, which may include answering questions or offering examples and connections to colleagues who have worked through similar challenges.
When asked what she might offer if teaching a new colleague to do this job, Karissa responded: “Each refugee family has an individual story even though some of them may come from the same country and camp. Don’t be afraid to ask them about their story and experience. Welcome them to our country and county.”
Ms. Pajau Vangay, PhD, contributed this article. RIHP staff consulted with Pajau as the Immigrant Microbiome Project team developed health education materials about nutrition and diet for refugees and immigrants.
The Immigrant Microbiome Project was an academic-community partnership built upon equity, inclusiveness, and shared values. This research project collaboration included the University of Minnesota; the Somali, Latino, and Hmong Partnership for Health and Wellness at West Side Community Health Services in Minnesota; and Chiang Mai University and the Shoklo Malaria Research Unit in Thailand. The research was conducted with 519 Hmong and Karen individuals living in Thailand and the Twin Cities metro area, including first- and second-generation immigrants and 19 Karen individuals sampled longitudinally, and 36 U.S.-born European American individuals.
Participants were asked to:
- Provide stool sample(s), dietary intake information, migration history, and demographic data
- Get measured on waist circumference, weight, and height
- Provide information on breastfeeding as a child, tobacco or alcohol usage, and medications
- Be excluded if they consumed antibiotics within the last 6 months, were regular users of probiotics, were pregnant, or were immunosuppressed
Community was central to the project, from its inception to the end. Members of the Hmong and Karen communities served on our boards as voices for their communities. They consulted on our study design, troubleshooted recruitment challenges, and helped us find ways to interpret our scientific findings into meaningful results. The Hmong and Karen community researchers were members of the research team from day 1. As trusted leaders in their communities, these researchers were critical to the successful recruitment of all of our study participants. The study results were published in 2018 (Cell: US Immigration Westernizes the Human Gut Microbiome). Researchers also created pamphlets (English, Hmong, and Karen) and shareable videos (English, Hmong, and Karen) for the broader community. In 2017, the team also offered Hmong Food Traditions Workshops to maintain health, and partnered with the University of Minnesota Extension: Expanded Food and Nutrition Education Program (EFNEP) to host nutrition and cooking classes in Karen.
Results:
- Hmong and Karen in Thailand were leaner and also had the highest gut biodiversity, compared to those in the U.S.
- Hmong and Karen gut microbiomes change within months of arriving in the U.S. and continue becoming more "Americanized" for decades
- Changes in diet explain some, but not all, changes in the gut microbiomes
We know that Hmong and Karen obesity risk increases after moving to the U.S., and now we know that their gut microbiomes change as well. There are many complex factors that contribute to obesity, and there are still many important questions to answer. These research results underscore the importance of preserving traditions not only for Hmong and Karen culture, but also for the potential to preserve Hmong and Karen microbiomes and health.
From January 1, 2018, through December 31, 2018, 818 primary refugees resettled in Minnesota. These included people with humanitarian immigration statuses – refugees, derivative and U.S.-granted asylees, parolees, Amerasians, and certified Victims of Human Trafficking. Among these, 787 were eligible for a post-arrival Refugee Health Assessment (RHA), typically initiated within 90 days of U.S. arrival, and 771 (98%) received an RHA. Components of the RHA include a health history and physical examination; immunization assessment and update; screening for infectious diseases; lead screening for children under 17 years; and assessment and referral for health problems including dental, vision, and mental health. Demographics, screening rates, and health summaries for 2018 primary and secondary refugee arrivals are available on the Refugee Health Statistics page.
From January to June 2019, 640 people with humanitarian immigration statuses arrived to Minnesota. The majority of arrivals were from Burma (39%), Democratic Republic of the Congo (19%), Eritrea (8%), Ethiopia (7%), and Ukraine (7%) (Figure 1).
Figure 1. Country of Origin of Primary Refugee Arrivals to Minnesota
January-June 2019* (N=640)
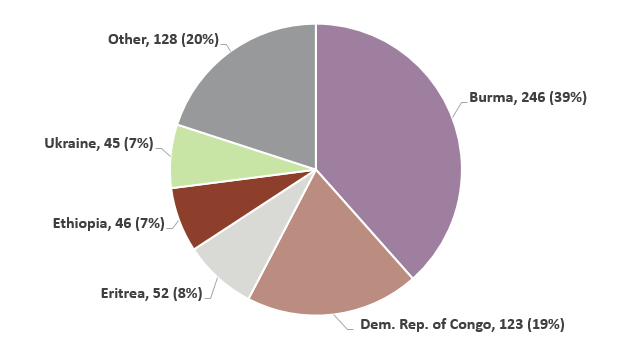 *2019 data are preliminary
Compared to previous years, the proportion of asylees, parolees, Amerasians, and certified Victims of Human Trafficking has increased due to the decreasing number of primary refugees (Table 1). In 2015, 98% of arrivals to Minnesota with humanitarian immigration statuses were primary refugees. In 2018, this proportion fell to 85%. Minnesota is continuing to see a higher proportion of asylees, parolees, certified Victims of Human Trafficking, and Amerasians in 2019.
Table 1. Arrival Status among Primary Refugee Arrivals to Minnesota
2015-June 2019*
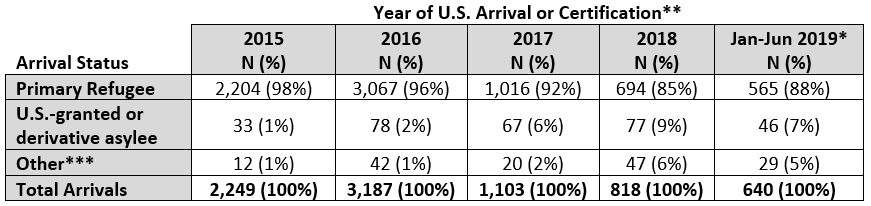 *2019 data are preliminary
**Year of U.S. arrival for primary refugees, derivative asylees, parolees, and Amerasians. Year of certification for U.S.-granted asylees and certified Victims of Human Trafficking.
***Includes certified Victims of Human Trafficking, parolees, and Amerasians.
|

