With spring in the air and the weather warming, the highest risk time for tick bites and tickborne diseases is here. Most Minnesotans who contract tickborne diseases are bitten by ticks from mid-May to mid-July.
The blacklegged tick, commonly known as the “deer” tick, is the most important of the dozen different types of ticks we have in Minnesota. The blacklegged tick transmits at least seven different disease agents to Minnesotans including the agents of: Lyme disease (caused by two different bacteria), anaplasmosis, babesiosis, one form of ehrlichiosis, hard tick relapsing fever, and Powassan virus disease.
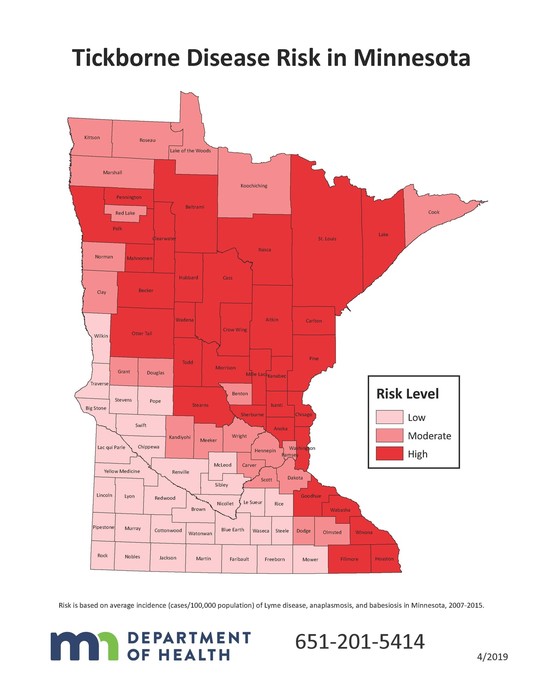
Blacklegged ticks have expanded their range within the state to include most of the forested regions of Minnesota. At the same time, the number of reported cases of tickborne diseases has increased dramatically during the last 20 years. The northeastern two thirds of the state is now considered high risk for tickborne diseases.
The best way to avoid tickborne illness is to avoid being bitten by ticks. Those who live in or visit wooded parts of Minnesota, especially during the spring and early summer, should take steps to avoid bites:
- Wear EPA-approved insect repellents and follow the manufacturer’s directions for application.
- Do frequent tick checks, looking at your body and clothes for ticks that are attached or crawling on you, especially in hard-to-see areas (e.g. behind knees, groin area, and arm pits).
- Remove any attached ticks you find on yourself as soon as possible. Grasp the tick with fingers or tweezers and pull outward slowly, gently and steadily.
Contact your doctor if you become sick (e.g., fever, rash, muscle and joint aches) within a month of a tick bite or visit to wooded areas.
For more prevention tips, print materials, videos, and more, check out www.health.state.mn.us/ticks.
On March 14, 2019, MDH facilitated a communication drill with community health boards (CHBs) and tribal health departments (THDs) across the state. The purpose of the drill was simple, MDH wanted to make sure there were at least three designated 24/7 emergency contacts for each CHB or THD entity. MDH used PartnerLink/MIR3, which is a mass notification system, to carry out this drill.
This drill was a no-notice event, meaning those 24/7 contacts had no advance notice of the drill. As least one person from each CHB responded to the notification. There were varying responses from the THDs ranging from all contacts responded to no emergency contacts responded. The largest gap identified was 24/7 contacts that had only their work phone number and email address in PartnerLink. The drill was conducted afterhours, so those that did not have mobile phone information in PartnerLink were not contacted.
MDH plans to continue to run these types of drills on an annual basis in order to improve our response capacity.
The Power of Storytelling
Public health is often an unseen force, working behind the scenes to protect and promote the health of individuals and populations. Part of the challenge when explaining the impact of public health to stakeholders is that we cannot always quantify our impact. This is especially true in public health emergency preparedness and response.
Project Impact seeks to provide state and local jurisdictions with tools to communicate the importance of the PHEP program. The Project Impact Website provides templates and tools for jurisdictions to tell their story and explain the importance of public health emergency preparedness funding.
Disaster Behavioral Health Conference: Footprint of Disasters Finding Strength
May 6
Earle Brown Heritage Center
Website and registration information.
Meta Leadership Workshop with National Preparedness Leadership Initiative
May 21
Earle Brown Heritage Center
Website and registration information.
|


