|
In Minnesota and across the United States, lead exposure and blood lead levels have decreased significantly in the last few decades. Yet lead exposure continues to compromise the health of many Minnesotans, and this is an area in which our state sees health inequities. The importance of this health issue is clear: there is no safe lead level, and high lead levels have been linked to neurological deficits, developmental challenges, organ failure, and death.
Recent immigration is a risk factor for lead exposure. Refugees may also experience other risk factors for continued exposure post-migration, including consuming imported goods (such as foods, spices, medicines/herbs, and cosmetics) and living in older homes. Because of the higher risk and prevalence of elevated lead levels among refugees, MDH recommends that every arriving refugee under the age of 17 be tested for lead within 90 days of U.S. arrival as part of the Refugee Health Assessment. Furthermore, following CDC Recommendations for Lead Poisoning Prevention in Newly Arrived Refugee Children, all refugees under the age of 6 should be retested within three months after resettlement in their permanent home, regardless of initial result.
The MDH Refugee and International Health Program (RIHP) and Environmental Health (EH) Lead Program conducted an initial data analysis and found that refugees from Afghanistan, Somalia, and Burma had higher rates of elevated lead levels—and lower rates of follow-up. To address these disparities, the RIHP and EH rolled out a CDC-funded initiative in early October 2018 to help understand and address the challenges that have led to comparatively poor follow-up rates among the refugee population.
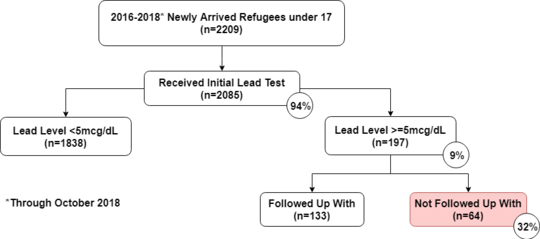
As part of this project, the RIHP and EH have completed a more comprehensive data analysis (see Figure 1). Of all refugees under 17 arriving between January 2016 and October 2018, 2,209 were successfully matched with the EH Lead Program’s surveillance system. Among those matched, 197 (9%) had initial elevated blood lead levels (EBLL); 64 (32%) of those with elevated levels did not receive follow-up.
Figure 1. Elevated Blood Lead Levels among Newly Arrived Refugees under 17
From this analysis, older children appear to be less likely to receive follow-up than younger children (see Table 1). MDH notified local public health and clinics about the 64 children who had not received follow-up, and they are currently being contacted and linked to care if possible.
Table 1. Refugees with Elevated Blood Lead Levels Lost to Follow-up by Age

While initial refugee screening rates are excellent in Minnesota, the next step of linking individuals to a primary care clinic requires active care coordination. Health care providers need to facilitate a warm hand-off referral to a primary care clinic if the family plans to change clinics after the Refugee Health Assessment. Compared to newly arrived refugees who have their initial health assessment at a primary care clinic, those who have their health assessment at a screening-only clinic have 2.04 greater odds of being lost to follow-up for elevated blood lead levels (see Table 2).
Table 2. Refugees with Elevated Blood Lead Levels Lost to Follow-up by Clinic Type

A strength of active lead surveillance is the remarkable work that counties and clinics do all across Minnesota. Because of the many systems involved (including the state, cities, counties, clinics, and laws governing rental housing), communication and tracking can be challenging. In February, the RIHP conducted interviews with 16 counties that receive refugees to identify gaps in the follow-up system, and we have been mapping the partners and processes that may affect lead follow-up. As an outcome of this initiative, we hope to capture and promote best and emerging practices across the state.
The joint RIHP-EH initiative is already leading to some concrete changes. The RIHP has been working with EH to increase the frequency of our data matching to identify individuals who need follow-up in a timely manner. To address a communication gap—MDH has traditionally sent reports to county lead case managers only for patients under six years old—EH will now send lists of children over six with elevated blood lead levels to local public health agencies. Refugee status will be indicated in those reports. EH is updating its lead education materials; the RHP will get these translated and prepare an education packet. Counties and clinics will then be able to download the packet for their patients. In addition, the RIHP will be updating the CDC Lead Tool Kit for Newly Arrived Refugees, a public resource for all providers who interact with refugees to learn how to best serve their communities.
If you would like more information regarding lead surveillance or ways to improve lead follow-up, please contact Katie Haugen in the MDH EH Lead Program at katie.haugen@state.mn.us.
Healthy Relationships and Domestic Violence
A collaboration of partners including the Karen Chemical Dependency Collaborative, Karen community members, Healtheast Roselawn Clinic, the Minnesota Coalition for Battered Women, and Twin Cities PBS (TPT) has jointly produced a new video on healthy relationships and domestic violence. The goal of the project was to describe the universality of domestic violence and discuss prevention and response tools, while considering adaptability of the content for other cultural groups.
Watch the video: Domestic Violence 101 Karen (YouTube) | English (YouTube)
Dr. Shana Sniffen of Healtheast Roselawn described the project: “This was truly a collaborative process with funding from several different agencies, content written by several Karen leaders, partnership with several domestic violence agencies, and animation by TPT. It was fun to work with so many different viewpoints and perspectives and to learn about the process of making an animated video from idea to script to images to storyboarding to voice recordings and finally an actual video. Hopefully, this video will serve as a learning tool to help Karen families be healthy and get the support they need.”
The Refugee and International Health Program provided some funding to help produce this short, cross-culturally accessible video, which will be integrated into our ongoing health promotion activities.
Multidrug-Resistant Tuberculosis (MDR TB)
It Took a Village! A community participatory approach to creating tuberculosis educational videos
Since January 2016, Minnesota has seen an increase in multidrug-resistant tuberculosis (MDR TB). This MDR TB outbreak is the largest of its kind in U.S. history and has disproportionately affected elders from the Hmong community living in the Twin Cities metro area. Tuberculosis (TB) is a bacterial infection, and it is transmitted through close contact with someone with active TB over a long period of time. To treat MDR TB, a combination of strong medications is required. MDR TB can be cured, but treatment can take between 18 and 24 months.
In response to the MDR TB outbreak, MDH’s International Health and Tuberculosis units reached out to the community to collaborate on a plan to address this serious health concern, and the Hmong TB Advisory Group was formed. Part of the response effort included the creation of an MDR TB educational video for the Hmong community. The goal of the video is to ensure that the Hmong community is well informed about what MDR TB is and how it can be prevented. The video is also intended to encourage people who have been exposed to MDR TB to seek a public health screening. From the start, it was clear that in order for the educational video to be effective in delivering its messages and reaching intended audiences, the Hmong community had to be an integral part of the video-making process.
To ensure that this was truly a community-driven effort, MDH staff collaborated with and sought advice directly from Hmong health care professionals, interpreters, and other community members. Before the video was produced, MDH incorporated health equity language into the call for proposals. Through information gathering at senior centers and with the Hmong TB Advisory Group, we learned about what kind of educational video the community wanted to watch and share. The primary audiences for the video are Hmong elders and their adult children or caretakers. Elders preferred a “Thai drama”-style video rather than a typical educational video.
During video production, the Hmong TB Advisory Group reviewed the video script (written by esteemed author Kao Kalia Yang) to ensure that the storyline was linguistically and culturally appropriate and the language and video style were consistent. Post-production, the Hmong TB Advisory Group reviewed and approved the video and provided guidance on the video dissemination plan.
Community engagement was essential to creating an educational video to address the MDR TB outbreak disproportionately affecting the Hmong community. MDH thanks the Hmong TB Advisory Group (which recently won a Ramsey County Public Health Award), as well as other key stakeholders and members of the Hmong community, for their contributions to the video.
Watch the video: Mob Kab Ntsws MDR TB (YouTube)
The Refugee and International Health website has moved!
New URL: https://www.health.state.mn.us/communities/rih/index.html
To better serve visitors to the Minnesota Department of Health website, we reorganized content, which changed the website links. Please update your bookmarks and links, and search the site to find what you need.
Do you know individuals who have had refugee status who are making contributions to the community? Nominate them to be recognized by the Minnesota Department of Human Services (DHS)!
The 2019 Outstanding Refugee Recognition Form is available online. You may nominate more than one person to be recognized as an Outstanding Refugee, but you must fill out one form for each separate nomination. The DHS Resettlement Programs Office will select nominees and recognize them during a ceremony in June 2019 as part of Refugee Recognition Month. The nomination deadline is midnight on April 19, 2019.
You may nominate individuals in one of three categories:
-
Entrepreneurship: Recognizes individuals contributing to their communities in business, the arts, or education.
-
Civic Engagement: Recognizes individuals making communities stronger through their civic participation.
-
Youth Achievement: Recognizes youth (age 20 or younger) who have achieved great milestones and/or are making a difference in their communities.
DHS launched the Outstanding Refugee Awards in 2017 to celebrate the strength, courage, and resilience of people who have had refugee status in Minnesota. Refugees are part of Minnesota’s rich immigrant history; since 1979 Minnesotans have welcomed more than 100,000 people with refugee status from 100 different countries. Refugees are people who have fled persecution and persevered through adversity. They need initial assistance when they come to Minnesota, but we often overlook the skills, ideas, and contributions that they make to our communities and our economy. They are earners and entrepreneurs, taxpayers, and consumers. These assets are wind in the sails of Minnesota’s growing economy, community, and cultural life.
The DHS Resettlement Programs Office is pleased to recognize individuals who are making a positive impact in our state, who once came with refugee status. Please share this widely and nominate an outstanding refugee in your community. Awards will be given in each region.
|


