 Rita Jensen, Case Aide at Anoka County Public Health, does a lot of work behind the scenes to make refugee health screening successful. When people with refugee status arrive in Anoka County, Rita connects with MDH, resettlement agencies, transportation services, clinics, and the newly arriving community members themselves to make sure they are connected to refugee health screening and care. Rita schedules appointments and follow-ups and helps troubleshoot if any appointments are missed. She has been in her current role for about six years and at Anoka County for nine years. She shares that she has felt very blessed in her work and in her team at Anoka County. We had a chance to chat with Rita before she retired on December 31.
“It’s a mixed feeling,” Rita says. The aspect of her work that she appreciates the most is the “satisfaction of helping these people who are coming from very difficult situations, and getting them through one of the first hurdles they have to deal with when they get to the U.S. and to Minnesota.” While much of her work is with a variety of partners and on the phone, her voice warms as she talks about interacting with newcomers. She recounts, “I worked with one dad whose wife and child were coming to join him. I got the luxury of meeting him in person, and he said, ‘I want you to meet my family, to come to my house for dinner.’” That gesture of hospitality and appreciation, even without a dinner being scheduled, has stayed with her through this work.
As Rita prepares to move on, she would advise those new to the work to be patient. "There are so many moving parts.” Communicating with people who may not speak English, who may be scared, or who may have a different understanding of punctuality for medical appointments and transportation is complex. Unexpected challenges “will happen and there’s nothing you can do to always prevent that, but you’re also going to get a lot of joy.” She says this job has touched her: professionally in terms of broadening the partners she connects with and the work she does, and personally in terms of a deeper understanding of difficulties people can face and appreciation for the freedoms in her life.
We wish Rita the best as she moves forward into retirement!
|
In Minnesota, we frequently refer to the “Refugee Health Screening” or “Refugee Health Assessment.” In actuality, the screening program serves a broader range of new Minnesotans. People are eligible for a refugee health screening if they hold an immigration status of refugee, asylee, certified victim of human trafficking, parolee, or Amerasian. These immigration statuses share a humanitarian basis.
More information on the definitions of each status:
U.S. Department of Health & Human Services: Office of Refugee Resettlement
U.S. Immigration and Customs Enforcement: Human Trafficking and Smuggling
It is important for providers to note that some or all of the clinical elements of the refugee health screening may be appropriate for patients with different immigration statuses, including citizens or undocumented persons. However, the refugee health screening program is designed for people with humanitarian immigration statuses, based on population-level health risks, and works both to protect the welcoming community and to promote optimal health for newcomers.
Eligibility for refugee health screening means several things. MDH RIHP works with local public health at the county level to coordinate screening, and screening results are returned to MDH RIHP for surveillance purposes (used to support refugee health in Minnesota and beyond). For a primary arrival (who came directly to Minnesota or who received their immigration status while residing in Minnesota) eligible for the screening, there may be funds available to cover the expense of screening if 1) the person has applied for and is ineligible for Medical Assistance, and 2) the screening has been initiated within 90 days of U.S. arrival or status certification. Please email Blain Mamo (blain.mamo@state.mn.us) with questions about this “flat-fee program” funding.
There are important differences between the eligible immigration categories:
- Case worker or case management services differ widely between immigration statuses. Derivative asylees, for example, who are often arriving from their original country to join a family member who was granted asylum, may not have a case worker.
- Primary refugees to Minnesota have an expedited application process for Medical Assistance. People with other immigration categories are not eligible for this, and their application process may be more challenging or lengthy.
- The process of applying for an immigration status varies by status. U.S.-granted asylees or certified victims of human trafficking applied for their statuses while living in the U.S. This means that they may already have employment and may already have established care in a health clinic. It also means that overseas screening information is not available for them.
- A person’s immigration experience, including any forced labor or trauma, can have serious impacts on their well-being and health. In some cases, specific additional screening may be appropriate based on this experience (for example, screening for agricultural toxins based on forced labor).
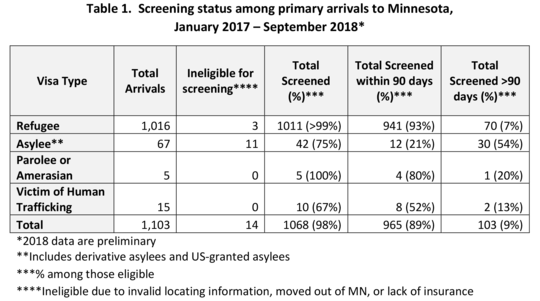
Data show that screening occurs at a higher rate and more promptly among people with refugee status in Minnesota as compared to those with other immigration statuses (see Table 1). This difference is particularly visible now, when people with refugee status make up a smaller proportion of those eligible for the refugee health screening than in years past, due to reductions in refugee resettlement at the federal level.
A prompt and high-quality health screening has the potential for an important positive impact on the lives of our newest Minnesotans. Some best practices for clinics and local public health shared by partners who work closely with asylees, victims of human trafficking, and others include:
- Work closely with caseworkers if available.
- Schedule the screening as soon as possible. Delays often lead to difficulty scheduling the screening because people have moved, changed their contact information, or become busier with employment and other commitments.
- For those without insurance who may be eligible for the flat-fee program, be aware of the 90-day screening initiation deadline. Reach out to MDH RIHP if assistance is needed.
- Be respectful and specific when introducing the purpose and benefits of the refugee health screenings. Be as flexible as possible if the client has already developed a rapport with a specific provider.
- If possible, verify the status of the Medical Assistance (MA) application. A client may have applied for a different benefit but not MA, or the filed application may not have been processed correctly.
An important milestone in the resettlement process is getting a “green card”—becoming a permanent resident, generally one year after U.S. arrival. The medical portion of the application to become a permanent resident requires the completion of the I-693 form by a federally designated civil surgeon (or, for refugees only, by a medical director for public health). This process is under federal jurisdiction. The I-693 examination is different from the refugee health screening: there are different clinical components; the I-693 is restricted in terms of which providers can conduct it; the exams take place at different times in resettlement; and they serve different immigration purposes. While the I-693 is beyond the jurisdiction of MDH RIHP, our program maintains a web page with pertinent updates and a list of civil surgeons in order to assist partners working with clients seeking green cards.
Recently, the Centers for Disease Control and Prevention (CDC) and U.S. Customs and Immigration Service (USCIS) issued new Technical Instructions for the I-693 and new processing protocols.
Key updates include:
- All applicants 2 years or older MUST have an IGRA TB test (not a TST).
- LTBI diagnoses through the I-693 should be reported to MDH within 30 days of I-693 completion, using the information and LTBI reporting form found in the Tuberculosis Screening section of the MDH website. While a release of information is not needed, patients should be informed of this referral.
- Due to processing changes, civil surgeons are encouraged to write the signature date on the outside of the envelope of a sealed copy of the I-693, to facilitate the client/lawyer in correct processing. Consider providing the client with an extra (unsealed) copy for their records.
Visit our website for more information and links to the full Technical Instructions and federal guidance: Minnesota Civil Surgeons
|


