|
In this edition of our newsletter, we give an
update on our mental health screening pilot project, with insights from Dr.
Georgi Kroupin of HealthPartners Center for International Health. We share
findings from a study, in which the MDH Refugee and International Health Program (RIHP) is a partner, on malaria awareness
among people visiting friends and relatives abroad. We also highlight data on
secondary refugee arrivals since 2010 and check in with Sarah Bluhm, the new
Program Manager supervising Catholic Charities’ refugee resettlement program.
Earlier this year, we covered the female genital
cutting (FGC) prevention project that MDH RIHP and partners are undertaking.
One component of this project is a grant program for community-based
organizations. Please see the grant announcement in this edition or the Minnesota
Female Genital Cutting Prevention and Outreach Grant Program page and share the
information with organizations that might be interested.
People who travel abroad to visit friends and relatives (VFRs)
often travel to high-risk destinations and may fail to seek pre-travel medical
advice. However, few formal studies have assessed the barriers to seeking
pre-travel care and perceptions of malaria risk among VFRs. MDH RIHP is a
partner in the Malaria VFR project, which aimed to describe the knowledge,
attitudes, and practices of West African VFRs traveling to malaria-endemic
countries.
We held eight focus groups with West African VFRs who live in the
Minneapolis-St. Paul area and eight additional focus groups with West African
VFRs who live in the Bronx, NYC. Our Community Advisory Board and partners reviewed
the themes generated from the focus groups, to ensure we stayed true to the
original intent of focus group participants’ statements. Ninety-two people joined the
focus groups and represented recent travel to five West African countries.
Many focus group participants said they considered malaria as they
prepared for travel, but described many barriers to pre-travel care and to
implementing prevention strategies while abroad. Barriers included:
- The high cost of provider visits and malaria-prevention drugs
- Challenges advocating for themselves in health care settings
- Concerns about offending people abroad by insisting upon
prevention practices that inconvenience local hosts
Cultural barriers to accessing care were also identified:
- Some participants lacked familiarity with the concept of
preventive care (vs. symptomatic or acute care), and participants cited hesitation
to ask health care providers for more information or explanation in pre- and
post-travel settings.
- Participants also expressed low confidence in U.S. providers due
to experiences with missed diagnoses or a perception that U.S. providers lacked
sufficient training to be a resource on malaria and other tropical diseases.
These focus groups confirmed that barriers to
adequate pre-travel care for VFR travelers to West Africa are multifaceted and
extend beyond VFR travelers’ perception of the importance of malaria prevention.
Interventions are currently taking shape, taking into account the role of
health care providers (both pre- and post-travel) and the need to address
system-level barriers to accessing care. Interventions will also build on community-based
programs to support malaria prevention behaviors and offer culturally
appropriate methods to encourage self-advocacy in health care settings.
Since starting the Secondary Refugee project in 2010, MDH RHP has been notified of
4,790 secondary refugee arrivals. The figure below describes the number of
notifications MDH has received each year (blue bars), the number eligible for a
health assessment (red bars), and the number who received a health assessment
in Minnesota (green bars). Overall, 52% of secondary refugees were eligible for
a health assessment in Minnesota, and 80% of those eligible received a health
assessment.
The number of secondary refugee notifications to
MDH peaked in 2015 (1,011) and fell to 551 in 2017, likely reflecting the lower
volume of refugee arrivals nationally. Eighty-eight percent of all secondary
refugee arrivals were Somali. The majority resided in Hennepin (39%), Stearns
(18%), and Kandiyohi (17%) counties.
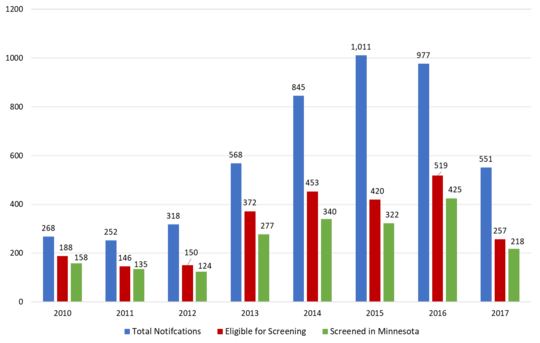
Figure: Secondary
Refugee Notifications to MDH, 2010-2017
Secondary refugees are individuals who initially settle in a state other than Minnesota but soon migrate to live in Minnesota. This migration can occur within days, weeks, months or a year of a refugee’s arrival to the U.S. Secondary refugees are eligible for a refugee health assessment if they have been in the U.S. less than one year and if they did not receive a health assessment in their primary state.
When local public health, a clinic, or a community-based organization is assisting a secondary refugee, they can complete a notification form and fax it to the MDH Refugee Health Program. (To request this notification form, send an email to Kailey.urban@state.mn.us.) The MDH RHP will then request the refugee’s overseas records, as well as domestic screening status and information, from the primary state, and forward that information to local public health.
Mental health screening belongs in the domestic Refugee
Health Assessment, as a part of overall health and well-being for any person,
and with special consideration for the challenges that refugees face from their
initial flight to building a new life in Minnesota. MDH RIHP and partners have
implemented a pilot screening process at four clinics, working toward an
effective, standardized way to address mental health in refugee health
screenings for adult primary refugees. For more information about the
background and beginning of this pilot, please see the article in the
January 2016 edition of the Refugee Health Quarterly.
Like other Minnesotans, people with refugee status may
experience a range of mental health challenges. The goal of the Minnesota
mental health screening pilot is to give health care providers an effective,
brief and simple tool for connecting with patients and assessing whether their
daily difficulties are related to mental health. The screening is designed to
identify those who may be in need of assistance, with mental health needs that
exceed their current coping abilities, regardless of the specific underlying mental
health diagnosis.
In addition, it was
important to build a set of questions that reflect experiences common for
people from different cultures and are easy to translate into different
languages. As Dr. Georgi Kroupin, Lead Mental Health Provider at pilot site
HealthPartners Center for International Health, explains, “It really helps a
lot to describe potential mental health problems in human terms, using lay
language that represents patients’ experience, not clinicians’ academic
training. The selected screening tool must be user-friendly for both providers
and patients and facilitate the provider’s engagement with the patient.”
In this pilot phase, MDH RIHP is working with partners to
finalize the screening questions. Currently, two similar but distinct sets of
questions are in use. MDH RIHP and partners are working to understand which
variation, or combination, best allows providers at diverse clinics throughout
Minnesota to work with and address the needs of their refugee patients.
Two sets of mental health screening questions currently used in
Minnesota pilot (note: differences are italicized)
Screening questions: HealthEast Roselawn, Hennepin County Public Health,
and Olmsted County Public Health
In the past
month, …
- Have you felt very sad?
- Have you been worrying/thinking too much?
- Have you had many bad dreams or nightmares?
- In the past month, have you avoided situations that remind you of the past? (PROMPT: Do you turn off the radio or TV if the program is disturbing?)
- Does any of the above stop you from doing things you need to do every day?
Screening questions: HealthPartners Center for International Health
In the past month, …
- Have you felt sad too much?
- Have you been worrying/thinking too much?
-
Have you had sleep problems? If yes, have you had many bad dreams or nightmares?
- Have you had memory problems?
- Does any of the above stop you from doing things you need to do every day?
Since January 2016, 947 screening results have been sent to
MDH RIHP from the pilot clinics, with 105 (11%) “positive” screening results;
55 (52%) of the 105 refugees accepted a referral for follow-up services.
Through pilot clinic
feedback, MDH RIHP has also refined the training and data collection processes.
Generally, the screening is considered “positive” if the patient gives two
“yes” responses. As with other health screenings, these results are evaluated in
the full context and clinical judgment of the provider, so a provider may note
potential mental health needs despite an otherwise “negative” screening result.
MDH RIHP is tracking the frequency and context of these cases. Through this
pilot, MDH RIHP supports partners in building on established mental health referral
best practices within diverse Minnesotan contexts.
This pilot supports the health of our newest
Minnesotans. Our aim is to remove potential barriers keeping people with
refugee status from contributing their best to their new communities, while improving
providers’ and health systems’ capability in addressing mental health with any
patient. Dr. Kroupin puts it this way: “The adopted screening process will be a
success when providers see it as useful and manageable … when it helps them to
see their patients as whole persons and to build better partnerships with their
patients.”

Sarah Bluhm is the
new Program Manager supervising Catholic Charities’ refugee resettlement
program. Sarah recently moved back to her hometown of Minneapolis after five
years at Heartland Alliance in Chicago as the Supervisor of Refugee
Resettlement Services.
“I’m thrilled to be
back in the Twin Cities continuing to do work that I love. In Chicago, I had
the opportunity to work closely with Rohingya, Iraqi, Syrian and Congolese
community members, and helped supervise one of the only LGBTQ-oriented programs
in the country. I am excited to work in the Twin Cities with the Somali and
Karen communities. One of the challenges of my role involves navigating the
services offered to refugees on a county-by-county basis. The populations we
work with here are much less centralized than I was accustomed to in Chicago,
where all of the services were centered in one county.
I’m really grateful
to see how welcoming and inclusive Minnesotans are towards our participants;
it’s something people truly take a lot of civic pride in. I’m also learning to
appreciate just how developed the health care support system in Minnesota is
for refugees. Every touch point my participants have with the health care
system, whether it’s finding a provider, or connecting them with an interpreter,
it all feels so integrated, making it easier to connect participants to the
care they require.”
|
Minnesota Female Genital Cutting Prevention and Outreach Grant Program
The Minnesota Department of Health will provide one-time grants to community-based organizations in Minnesota communities that are impacted by female genital cutting (FGC), supporting community-led efforts to educate and inform communities about the health risks and emotional trauma inflicted by FGC practices and the criminal penalties associated with FGC. Organizations may propose educational programs, media campaigns, community conversations, and/or other engagement efforts related to FGC prevention in their Minnesota communities.
Find the Request for Proposals (RFP), more information and FAQ here: Minnesota Female Genital Cutting Prevention and Outreach Grant Program
Deadline: Friday, April 27, 2018
Please share widely with anyone who may be interested. Thank you!
Refugee Recognition Month 2018 Poster Contest
As part of Minnesota’s June
Refugee Recognition Month, you are invited to help design the 2018 Refugee
Recognition poster which will be displayed on the Department of Human Services
(DHS) website during June. The DHS Resettlement Office is seeking young artists
who can illustrate the “Courage and Hope” that it takes to start over in
Minnesota by creating an image for the June poster design.
Please submit an original
picture or image of what Refugee courage and hope means to you.
2018 Theme: Courage and Hope.
Deadline: May 4, 2018
Parameters: 11x8.5 size –
landscape orientation
Photos: 330 PPI high quality
resolution
Graphics: vector based, CNYK
color mode
Eligible artists: school aged
young people up through high school. Preference given to artists who have had
refugee status or are the children of refugees.
Images can be scanned and sent to: Seble Doble, seble.doble@state.mn.us
Or
mailed:
ATTENTION Seble Doble, MN Dept. of Human Services, PO Box 64961, St. Paul, MN
55164-0951
|


