Happy 2018! We’re looking forward to a
productive and healthy year. In this edition, we give you updates on our most
current refugee arrival numbers, information on a new Female Genital Cutting
Prevention initiative we have undertaken, and a reminder about the specific
Adjustment of Visa Status medical exam (Form I-693) requirements for refugees.
In December 2017, the Refugee and International
Health Program welcomed Mimi Ahmed Mohamud as our International Health
Communications and Engagement Planner. She will consult with various MDH
programs on Limited English Proficiency (LEP) communication strategies and
coordinate health promotion messaging with diverse local media outlets. Mimi
will also assist with identifying needs and improving engagement and communication
with LEP communities. She has a Master’s of Public Health with a concentration
in Global Health from St. Catherine University, where she also received a
Bachelor’s of Science in Public Health with emphasis in Public Policy.
Previously, Mimi was a WIC nutrition educator. She also worked as a tobacco
control program manager, providing technical assistance to grantees in
Minnesota working in tobacco control and managing smoke-free policies grants
for select Minnesota counties. Mimi looks forward to working with our many
RIH partners and communities!
|
The United Nations has designated February 6 as the
International Day of Zero Tolerance for Female Genital Mutilation (#EndFGM).
The issue of female genital mutilation/cutting (FGM/C) taking place
received attention in the U.S. this past year when a Detroit-area doctor was charged
with mutilating genitals of two Minnesota girls.
Minnesota has had a law banning FGM/C since 1994
(even before federal legislation outlawed FGM/C in 1996). In the 2017
legislative session, the Minnesota House approved a bill
that would make it a felony for parents to allow their children to undergo
FGM/C (HF 2621 4th Engrossment). The bill had a number of provisions that could remove children from
their parents’ custody, or terminate parental rights, in cases of FGM/C. After
hearing concern from communities about the potential for breaking up families
and discouraging families from seeking health care, the Senate did not move
forward with its version of the bill (“Minnesota
bill against female genital mutilation raises opposition”).
Many community advocates favor a less punitive
approach to FGM/C prevention, emphasizing education and community engagement.
MDH RIH is partnering with the International Institute of Minnesota to form the
Minnesota FGC Prevention and Outreach Working Group. The main goal of the group
is to identify and develop effective prevention and outreach strategies for
Minnesota communities. The group will develop recommendations for FGC
prevention among Minnesota communities. Working group members will represent a
variety of roles and sectors, such as community leaders, health care providers
and government agencies.
The working group is part of an FGC prevention
project sponsored by the Minnesota Department of Human Services. The project
also includes a one-time grant opportunity for community-based organizations to
do FGC prevention work. MDH RIH will publicize the Request for Proposals widely
when it goes live in a few months.
If you would like to learn more about the
Minnesota FGC Prevention and Outreach Working Group, or recommend a person or
organization for membership in the group, please contact Ann Linde at ann.linde@state.mn.us.
Minnesota resettled 3,186 primary refugee arrivals in 2016.
The majority of these arrivals were Somali (45%), Burmese (21%), or Ethiopian
(9%). These refugees resettled in 24 counties in Minnesota, with the largest
number resettling in Ramsey County (N=1,467), Hennepin County (N=631), Stearns
County (N=281), and Anoka County (N=192).
Among these, 3,125 were eligible for a post-arrival Refugee
Health Assessment (RHA), typically initiated within 90 days of U.S. arrival. 3,101 (99%) received a RHA. Components of the RHA include a health history
and physical examination; immunization assessment and update; screening for infectious
diseases; lead screening for children under 17 years; and assessment and
referral for health problems including dental, vision and mental health.
Demographics, screening rates, and health summaries for 2016 primary and
secondary refugee arrivals are available at Refugee Health Statistics.
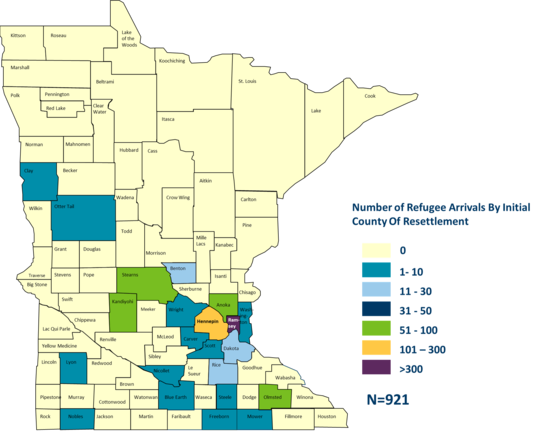
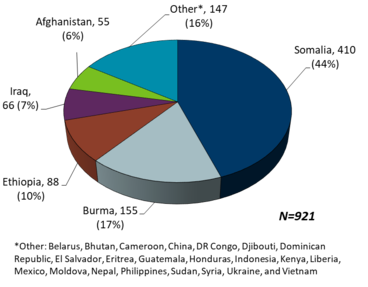
From
January to September 2017, 921 primary refugee arrivals resettled in Minnesota.
The county of resettlement is described in Figure 1, with the largest
proportion (40%) resettling in Ramsey County. The country of origin of these
arrivals is described in Figure 2, with Somalis comprising the largest
proportion (44%). During this time period, the RIH program also received
notification of 463 secondary refugee arrivals, a 40% decrease compared to
the same time period in 2016. The majority of secondary arrivals were Somali
(92%).
Figure 1. County of Resettlement of Primary Refugee Arrivals to Minnesota, January - September 2017
Figure 2. Country of Origin of Primary Refugee Arrivals to Minnesota, January - September 2017
After being in the
United States for one year, refugees are eligible to apply to adjust their
status to Legal Permanent Resident (or get a "green card”). This
application includes form I-693, the Report of Medical Examination and
Vaccination Record (USCIS: form I-693). Although the adjustment of status process
falls beyond the initial resettlement period, refugee health partners at
clinics, counties, and resettlement agencies frequently receive questions and
requests related to the process.
There are some
important differences between the I-693 requirements for refugees and all other
groups of immigrants. Refugees without a Class A condition (which includes very
rare conditions that involve a waiver and additional examination) only need a vaccination
review and a signature from either a Civil Surgeon or the medical director
of a county. Other groups of immigrants need both a medical examination and
vaccination review, and a signature from a federally designated Civil Surgeon.
Dr. Robin Molella completes
I-693 forms for refugees as the medical director of Olmsted County as well as
for other immigrants as a provider and Civil Surgeon at Mayo Clinic. She feels
passionately about this service. Speaking to her role at the county level, she explained,
“[Offering I-693 completion for refugees] is not without demands on staff time,
but it has real value for the jurisdictions as well. This assures that refugees
reconnect with local public health, have a high-quality immunization review and
build trusting relationships with public health. Given the
vulnerability of refugee populations to a wide range of health threats,
nurturing this relationship is critical. Staff costs can be offset with
moderate fees.” Those same considerations apply in the context of a primary
clinic or health care home as well. Dr. Molella noted that the human impact of
this service, and the difference it makes to people and families to be able to
adjust their immigration status without additional barriers, is enormous.
For many newly
arriving refugees in Minnesota, the process of the refugee health exam soon
after arrival involves the assistance of resettlement workers, local public
health and clinic staff. Completing the medical section of their green card
application is very different: families often must find their own way through
the system. In addition, an administrative fee (not covered by insurance) is
usually charged and can vary widely among providers. This can pose a financial
barrier, especially for large families. Individuals and families may need to
travel to another county or part of the state for their required appointment, as
many areas of Minnesota have a Civil Surgeon shortage. (See the list of Civil
Surgeons at Minnesota Civil Surgeons or USCIS:
Find a Doctor.)
Any
doctor interested in becoming a Civil Surgeon, or Medical Director interested
in offering I-693 processing, may get more information at the United
States Customs and Immigration Service Dedicated Civil Surgeons webpage.
 Patty Seflow retired this month, after working for 16 years as a public health nurse in Ramsey County. She has been a longtime partner of RIH through her role in the TB clinic working with refugees and immigrants. We wish Patty well in her next adventures! (Responses have been edited for length.)
Q. Please share how you first got involved working in public health.
A. In 1980, I volunteered with the American Refugee Committee to work in Ban Vinai Refugee Camp, a camp for Hmong refugees in northern Thailand. I worked in a pediatric ward of the hospital, where we saw many children with severe gastrointestinal and respiratory conditions. Most disturbing was the special room in the hospital for babies with tetanus. Our treatment modalities were very limited: IV fluids, basic antibiotics and two oxygen tanks which had to be shared among the most critically ill children with severe respiratory conditions. It was pretty overwhelming for this nurse who had been working on a pediatric unit at the University of Minnesota Hospital! From my walks around the camp and speaking with other expatriates with many years of experience working in similar conditions, it became clear that, after treating them, we were sending the children back to the environment which had caused their illness. Clean water, adequate sanitation and immunizations would accomplish far more in keeping children healthy than the best tertiary care. In other words, basic public health measures – prevention, rather than treatment. That set my career path. I came home, quit my job at the University of Minnesota Hospital and starting working for, at that time, the Ramsey County Public Health Department as a Public Health Nurse.
|
Q. What were some challenges and successes in your public health work?
A. A perennial challenge is informing the public about the good work that we do. As has been said, “public health is a well-kept secret.” People are not aware of the many ways that public health work touches their lives. Because much of public health work depends on tax dollars, it’s important that the public understands what their tax dollars pay for. As an example, in the case of an active TB case in a worksite, TB Clinic staff will often offer screening at the worksite (convenient for the employees and efficient for TB staff). At the information meeting with the employees, the question of cost to the employees always arises. I am happy to respond that the screening is free to the employees, saying, “This is your tax dollars at work – an example of protecting the health of the public.”
A great success was moving the screening of refugees from the health department to private clinics. There was some anxiety that refugees would be “lost” and not receive this essential service. However, we have a dynamite nurse who fully embraced the work and became the hub of contact for our partners in this work: voluntary agencies sponsoring the refugees, private clinics doing the screening, transportation companies and MDH. With her leadership and the work of our partners, we consistently achieve screening rates of 98-99%.
Q. What is your proudest moment at Saint Paul-Ramsey County Public Health?
A. I am most proud of the patient-centered care we provide our patients. As a referral clinic (“we call them, they don’t call us”) that serves people from many countries and cultures (and we are addressing a condition which can cause fear, anxiety and/or denial), it is a necessity that we meet the patient where they are. Staff are skilled listeners and patient educators. We do reminder calls, failure calls, arrange transportation, do home visits and generally allow for “flexible appointments” (patients have appointments, but, for some patients, these are mere suggestions. We still see them when they present to the clinic). The success of this work is reflected in our completion rates for patients with latent TB infection and the successful completion of treatment for patients with active TB disease.
Q. What do you wish other people knew about working with immigrant populations?
A. Working with immigrant populations presents some challenges – differences in language, culture, understanding and acceptance of the Western health care system, etc. However, all people want to be healthy. All cultures have different modalities of “prevention of disease,” whether it’s a special tea or a special medallion worn around the neck to ward off spirits. All cultures have treatments for disease. The challenge is to recognize and respect the patient’s beliefs and history, while making an effective case for the Western way of prevention and treatment. And what an interesting road that takes you on! The reward vastly outweighs the effort.
Q. What changes would you like to see over the next five years?
A. I would like to see a greater societal recognition of the potential of immigrants and refugees. I recall, when working in a refugee camp on the Thai-Cambodian border, a volunteer surgeon from the U.S., working in our small surgery ward (dealing primarily with wounds, abscesses, fractures), said to me, “The medics and nurses working on the ward are amazing. They survived the Khmer Rouge, had their education interrupted and still they do great work on the ward. The head medic is smarter than I am. He could do anything he wanted in the U.S.” That is the case with so many refugees and immigrants. They still believe in the American dream and are willing to work to achieve it. Our small role is to help assure their health needs are identified upon arrival through a health screening, and in the case of latent TB infection, successfully treated.
Q. What are some memories you will take with you?
A. It’s always memorable when a patient with active TB disease completes treatment, especially if the course of treatment was fraught with difficulties (denial of disease and resistance to treatment, side effects to the medications, etc.). One patient, in particular, comes to mind. We celebrated her completion of a one-year treatment course by giving her a fruit basket. She rewarded us with a little dance down the hall in the TB clinic.
The memories I take with me could fill a book. Sixteen years of working with dedicated, committed staff who go the extra mile for our patients; and many, many interesting, delightful patients. I have never lacked for interesting work and I have never had to look for meaning in my work. Who can ask for more in a career?
Q. What legacy do you leave behind?
A. I’m confident that through the work of the refugee and TB programs at the Saint Paul-Ramsey County Health Department, refugees have an opportunity for a healthy start to their life in the U.S., and many cases of active TB have been prevented.
Q. Now that you are retiring, what are your plans?
A. I will just quote Dr. Seuss: “Oh, the places you’ll go! There is fun to be done!”
|