|
The much-anticipated Presidential Determination on Refugee Admissions for Fiscal Year 2018 was issued on Sept. 29, 2017. The admissions cap is set at 45,000, and we expect a proportional reduction in arrival numbers in Minnesota. At this time, the demographic details of the refugees destined for Minnesota are unknown.
Despite slow arrivals, our program continues to work on various refugee and immigrant health initiatives. In this edition of the newsletter, we highlight the interactive health lessons for English learners that recently went live on our website. We also feature the work of the Karen Chemical Dependency Collaborative (KCDC), our community partner, which launched the Karen Recovery Program and is now accepting referrals. Our MDH colleagues in the Sage programs discuss their exciting partnership with International Medical Graduates (IMGs) in a project designed to increase cancer screening rates in refugee and immigrant populations. We recently evaluated measles, mumps, rubella (MMR) immunization coverage among asylees; we’ve included a summary of the findings.
We encourage our partners near and far to attend and submit proposals to the North American Refugee Health Conference, June 7-9, 2018, in Portland, OR. The call for abstracts is now open!
The Karen Chemical Dependency Collaborative (KCDC) is a cross-professional, cross-cultural collaboration that began in 2013 when a group of providers and Karen community leaders identified substance use and its associated consequences as the greatest unmet need facing the Karen community. At the time, there were no culturally specific treatments for Karen people. KCDC is focused on improving substance-use related services with four broad initiatives:
- Developing culturally/linguistically relevant community education materials.
- Developing culturally specific substance use treatment.
- Training Karen interpreters on mental health and substance use terminology.
- Training Karen faith leaders to support individuals and families struggling with substance use problems.
In September 2016, KCDC launched the Karen Recovery Program at HealthEast in collaboration with the Karen Organization of Minnesota. The program currently offers culturally specific outpatient treatment for Karen men. KCDC has implemented a weekly AA-style community support meeting led by a Karen facilitator; developed several community health education materials, including a video on DWIs developed with the City of Maplewood; and created Toh Moo: Karen Resources, a bilingual resource website searchable in English and Karen.
KCDC has trained 77 Karen interpreters and held four meetings with Karen faith leaders to build their capacity to support Karen families dealing with substance use problems. KCDC has begun working with an adolescent substance use treatment center to adapt its services to be culturally relevant for Karen youth. KCDC holds bimonthly meetings and welcomes all stakeholders. Referrals for the Karen Recovery Program can be made to Tonya Horn, HealthEast Roselawn Clinic, 651-326-5743 or tlhorn@healtheast.org.

Leadership team of the Karen Chemical Dependency Collaborative:
Ehtaw Dwee, Dr. Shana Sniffen, Paw Wah Toe, Ta Da, and Tonya Horn
Like refugees, asylees are unable to return to their country of origin due to persecution based on their race, religion, nationality, membership in a certain social group, or political opinion. Asylum is granted after they arrive in the United States. An asylee can also apply for family members to enter the U.S. as derivative asylees. Overseas medical records for asylees are forwarded to our Refugee Health Program. Asylees and derivative asylees are eligible for the domestic refugee health assessment (RHA), but because they do not receive assistance from refugee resettlement agencies, there is concern that asylees may be missing opportunities to connect to health care.
We analyzed measles, mumps, and rubella (MMR) vaccination coverage for the 2,023 asylees (112 U.S.-granted and 1,911 derivative) who arrived in Minnesota from 1999 through January 10, 2017 as a surrogate measure of whether this population was accessing health care. Immunization data were from the Minnesota Immunization Information Connection (MIIC), Minnesota’s immunization information system. Completion of the MMR vaccine series occurs when an individual receives two doses of the vaccine after age 12 months that are given at least 28 days apart. Ideally, the first dose is given when a child is between 12 and 18 months of age, and the second dose is given between 4 and 6 years of age. Asylees are often on the catch-up vaccination schedule. Individuals born before 1957 are considered immune and generally do not need to be immunized unless they work in certain health care environments.
Overall, 1,223 (60 percent) of asylees completed their two-dose MMR series (Table 1). Among those who completed the series, about half started the series overseas (48 percent), with very few (7 percent) completing the series prior to U.S. arrival. However, 75 percent of those who completed the MMR series did so within a year of arrival. Of those who did not complete the MMR series, only 18 percent started the series overseas. Children ages 6 through 18 years had the highest overall MMR completion rate (73 percent). Although 78 percent of adults ages ≥19 years had received at least one valid dose of MMR either overseas or domestically, this group had the lowest overall MMR completion rate (42 percent).
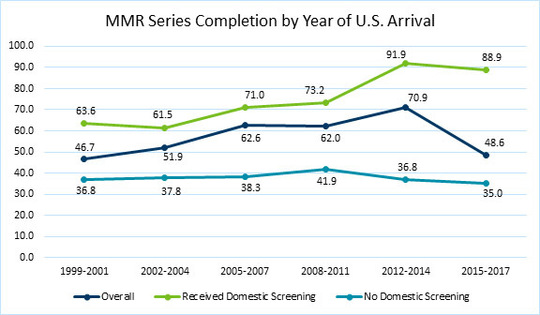
There was a marked difference in MMR completion rates between those who received a domestic RHA (72 percent) and those who did not (38 percent). MMR completion rates steadily increased over time, from 47 percent for arrivals between 1999 and 2001 to 71 percent between 2012 and 2014 (Figure 1). Recently, however, only 49 percent of arrivals between 2015 and January 2017 have completed the MMR series. This could be because only 46 percent of these asylees have completed their RHA. Additionally, these asylees have spent less time in the U.S. and may not have had sufficient time to complete the series.
This evaluation highlights the importance of the RHA as an opportunity for asylees not only to receive important health services, such as immunizations, but also to establish ongoing care. The adjustment-of-visa medical exam that generally occurs one year after residency in the U.S., as well as school enrollment requirements, offer additional chances for asylees to get immunizations. Our data show a need to address barriers that affect access to health care for asylees (insurance, transportation, etc.). Ensuring the completion of the RHA among asylees would help increase their immunization rates, especially among adults. We will continue to monitor this trend to ensure that eligible asylees are connected to care.
Table 1
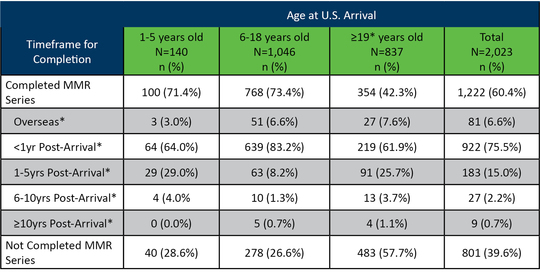
Figure 1
The Minnesota Department of Health Sage Programs provide cancer screening services for thousands of Minnesotans annually, including the state’s growing refugee and immigrant populations. Sage partners with a network of over 460 clinic sites to reduce the burden of cancer by providing uninsured and underinsured populations access to free breast, cervical, and colorectal cancer screening services. Sage serves a very diverse clientele, with over 70 percent from populations of color. Since 1991, more than 160,000 individuals have received free cancer screenings through Sage.
Sage Programs has a new and exciting collaboration with International Medical Graduate (IMG) physicians to improve cancer screening rates for Latino and East African communities in Minnesota. This partnership was designed to address health disparities in Minnesota’s refugee and immigrant populations. After an initial period of training and shadowing Sage staff, IMG physicians—medical graduates in their home countries who have not yet been licensed in the U.S.—are matched with Federally Qualified Health Centers in need of patient navigators. IMG physicians address access issues and fears about cancer screening. Currently participating IMG physicians speak Somali, Oromo, Amharic, and Spanish. The IMG physician navigation partnership has received strong praise from Sage patients who report that they are much better able to connect with physicians who understand their language and culture.
Get more information on Sage Cancer Screenings Covered Services & Eligibility or by calling Sage navigators at 1-888-643-2584. Sage staff are fluent in English, Spanish, Hmong, and Vietnamese; additional languages are available via Language Line free of charge.
Have you seen our #RefugeesOfMN posts on the Minnesota Department of Health Facebook page? These posts share stories from Minnesota refugees on what health means to them. Our July post featured Pakou Hang, a Hmong refugee and co-founder of Hmong American Farmers Association.
We’ve added two lessons to the online MDH health curriculum for English learners: Mental Health and Immunizations. Learners can engage with these lessons in a new, interactive format (a PDF option is also available). The curriculum may be used by learners independently or in adult education classrooms. It’s appropriate for high-intermediate and advanced English learners.
Check out the interactive lessons and the whole curriculum at English Language Learners (ELL) Health Curriculum.
We welcome your feedback and would love to know if you’re using the lessons! Let us know if there are topics you would like to see added, as we hope to expand the curriculum. Contact Ann Linde at ann.linde@state.mn.us.
|



