|
Our staff kicked off the summer by attending the North American Refugee Health Conference held in Toronto. There were inspiring discussions on refugee health services, compassion in medicine, the resilience of Syrian refugees in Canada, and much more. We, along with our Center of Excellence in Refugee Health partners, gave various poster and oral presentations and led workshops highlighting our quality improvement projects and guideline development work:
- Feasibility of using health care claims files for refugee child epidemiology
- Health surveillance of refugee children using state records
-
Demographics, domestic refugee health assessment history, and clinical risk factors among Minnesota primary refugees diagnosed with tuberculosis (TB) disease, 1993-2016
- Linkage to care for newly arriving refugees infected with hepatitis B Virus
-
Using the electronic health record to enhance the refugee health examination for new arrivals to the US
-
Engaging partnerships: Overseas and domestic systems collaborating to receive refugees with significant health needs
-
Clinical case management of parasitic infection refugees after arrival in light of pre-departure presumptive treatment
Next year’s conference, sponsored by the Society of Refugee Health Care Providers, will be held on June 7-8, 2018, in Portland, Oregon.
In honor of World Refugee Day, we debuted a series of profiles of refugee community members, in which they share their views on health and life in Minnesota. Find posts featuring Husein Yussuf and Pakou Hang (with more to follow) on the MDH Facebook and Instagram accounts. Follow along and post your own stories with the hashtag #RefugeesofMN.

 Pictured, left to right: Donna Jorgenson, Sharon Traen, Tracy Luchsinger, Ellen Frerich (MDH), Anna Terry
Tracy Luchsinger, a physician assistant at the Allina
Burnsville clinic, was recently honored as a runner-up for the Dakota County
Public Health Achievement Award. In their nomination letter, the public health
team at Dakota County writes about Tracy’s “tireless and fabulous work with our
refugee clients,” both in the initial refugee health screening and in ongoing
care for patients. They write, “we trust her to care for our newly arrived
refugees with compassion, wisdom and skill.” Tracy says that she enjoys “completing
refugee physicals as they are an important tool to ensure these individuals are
screened for high risk conditions that we, as Americans, typically don't have
to worry about, or are routinely tested for and caught early.”
 |
Our division is in the midst of the CDC-funded Malaria
Project, in collaboration with the University of Minnesota, HCMC, HealthPartners,
and other national partners. The number of individuals diagnosed with malaria
in the U.S. has increased in recent years. Since malaria is not endemic in the
U.S., travelers who visit friends and relatives in malaria-endemic regions are the
most susceptible. This project aims to determine whether U.S. residents
traveling to these regions are taking preventative measures before leaving—and
if not, why? How can we help these travelers stay healthy when abroad?
We held a community forum on Saturday, May 6, 2017 at the
Brooklyn Park Community Activity Center. The main goals of the forum were to
share malaria information and resources, inform community members about the
next steps of the project, highlight the community advisory board and partner
community organizations, and present findings from the eight focus groups held
in the Twin Cities.
The findings from the focus groups often differed from the
anecdotal assumptions that travel doctors make about travelers who are visiting
friends and relatives. As cited in the literature, many travelers view cost as
a major barrier to accessing malaria medications. The out-of-pocket expense is
too high, even for those with Medicare or Medicaid. This was the most common
barrier identified in the focus groups, and forum attendees strongly agreed
that this was an issue.
The focus groups also identified barriers
that are not cited in the literature. For example, travelers did not want to
inconvenience their hosts with special requests such as bed nets or staying
indoors at dusk, when many are outside to socialize. While many participants
recognized the need to protect themselves from malaria (counter to the common view
that these travelers believe they are at a lower risk for malaria and do not
need to protect themselves), the need to respect their hosts and avoid being
perceived as “too American” can be more important.
The forum provided the opportunity for attendees to dialogue
with study staff and partners. It was a great opportunity to report back to the
community and share malaria information. Thank you to everyone who joined us!
Secondary refugees are individuals who initially settle in a
different state but soon come to live in Minnesota. The Refugee Health Program
does not currently have a systematic way of capturing all secondary migration
data. We are most often notified of a secondary refugee’s arrival by local
public health, a refugee resettlement agency, or a clinic. We started receiving
referrals in 2016 from community-based organizations (CBOs) that assist refugee
populations. You can find a list of Minnesota CBOs in the 2016-2017
Directory of Refugee Service Providers.
When we are notified of a secondary refugee arrival, our
staff requests copies of the overseas medical records and U.S. screening
history from their primary state. We share this information with the local
public health jurisdiction where the refugee is residing. Local public health
partners work with clinics to ensure that eligible secondary refugees receive
health screenings. We established these screening eligibility criteria for
secondary refugees: they can seek a refugee health assessment if they have been
in the U.S. less than one year, if they did not complete a health assessment in
their primary state, and if they have medical insurance.
In
2016, the Refugee Health Program was notified of 977 secondary refugee
arrivals, including 350 (36 percent) who had arrived in Minnesota ≤90 days
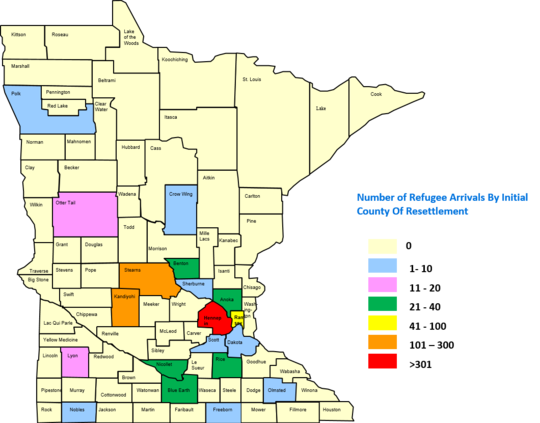
after U.S. arrival. Ninety-one percent of secondary arrivals were Somali. Figure 1 shows that the
majority resettled in Hennepin County (N=346), Stearns County (N=225), and
Kandiyohi County (N=135).
Figure 1. 2016 Notifications of Secondary Refugee Arrivals
to Minnesota by County
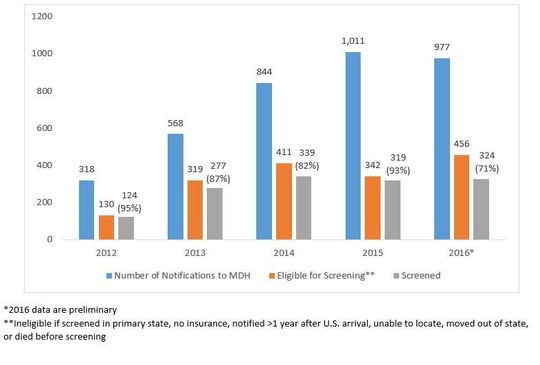
Four-hundred fifty-six (47 percent) were eligible for a screening in Minnesota, and screening results have been submitted to the RHP for 324 (71 percent) of those eligible (Figure 2). The remainder are in the process of being contacted for a screening, or they have been screened and the results have not yet been submitted.
Figure 2. Notifications of Secondary Refugee Arrivals to
Minnesota, 2012-2016*
|

