|
To: Maine Immunization Program Providers
From: Maine Immunization Program
Subject: RSV Webinar Invitation - Updated Guidance for the Remaining of Respiratory Syncytial Virus (RSV) Season and Planning for Next Fall
Date: February 1, 2024
The Maine Immunization Program would like to provide updated guidance and best practices for Respiratory Syncytial Virus (RSV) prevention.
Last week, the Maine Immunization Program opened ordering to all enrolled Vaccines for Children (VFC) providers for doses of 50 mg nirsevimab after fulfilling the orders for the birthing hospitals. With an increase in the state allocation of nirsevimab 50 mg doses, the maximum order quantity is now 50 doses per order, until the supply is exhausted. Please only order what you anticipate using by the end of RSV season (March 31, 2024) for infants. The current stock of nirsevimab 100 mg has been claimed by our enrolled VFC providers and is no longer available for order in ImmPact. Please reach out to MIP if you find there is a need for additional doses.
All nirsevimab products in the State of Maine have an expiration date ending in 2025. Any inventory remaining after this cutoff date should continue to be stored at appropriate temperature and monitored until next RSV season. Should practices that are only carrying nirsevimab not wish to continue monitoring and housing this vaccine, MIP can arrange transfers.
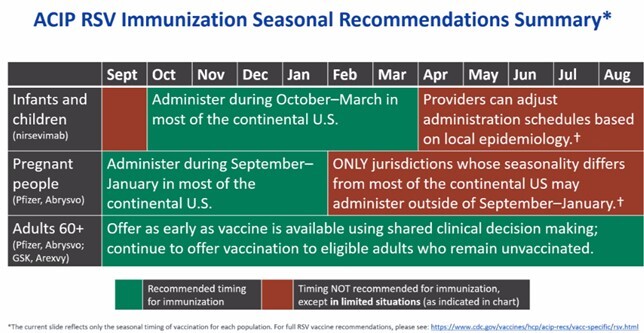
Each age group has a recommended timing for immunization during the respiratory season. The Advisory Committee of Immunization Practices (ACIP) has provided a detailed chart showing recommended timing of immunization for each population. Note that the deadline for administering RSV vaccine for pregnant people was January 31, 2024. Infants and children should receive nirsevimab until March 31, 2024.
The Maine Immunization Program will be hosting a lunch and learn webinar on February 8, 2024 @ 12:00 PM, focusing on updated guidance for Respiratory Syncytial Virus (RSV) prevention for the remainder of the 2023-24 RSV season and preparing for next fall. We are pleased to be joined by experts from the manufacturer, Sanofi, to discuss nirsevimab (Beyfortus) for infants and young children. Topics will include recommendations from the Centers for Disease Control and Prevention (CDC) for use of nirsevimab, timeframes of RSV season, and planning for the next RSV season. We invite providers to join us for this exciting opportunity to learn more about RSV prevention.
Call information: Maine Immunization Program is inviting you to a scheduled Zoom meeting.
Topic: RSV Webinar Invitation – Updated Guidance for Remaining of Respiratory Syncytial Virus (RSV) Season.
Join Zoom Meeting: https://mainestate.zoom.us/j/84248006212?pwd=bUMyYlRJNldzNm1od0JjSUxuSjRLdz09
Meeting ID: 842 4800 6212
Passcode: 65057837
One tap mobile +13863475053,84248006212# US
The Centers for Disease Control and Prevention (CDC) issued three COCA Now messages in January 2024. The COCA Now provides updated guidance for the use of nirsevimab for young children, information on administration errors in young children and pregnant people, and recommendations for the end of maternal RSV vaccine season.
COCA Now: January 5, 2024
|
Updated Guidance for Healthcare Providers on Increased Supply of Nirsevimab to Protect Young Children from Severe Respiratory Syncytial Virus (RSV) during the 2023–2024
Respiratory Virus Season
|
|
On October 23, 2023, the Centers for Disease Control and Prevention (CDC) issued Health Alert Network (HAN) Health Advisory 499 to provide guidance for prioritization of nirsevimab given limited supply. Nirsevimab (Beyfortus, Sanofi and AstraZeneca) is a long-acting monoclonal antibody immunization recommended for preventing RSV-associated lower respiratory tract disease in young children. Given the recent increase in nirsevimab supply and the manufacturers’ plan to release an additional 230,000 doses in January, CDC advises healthcare providers to return to recommendations put forward by CDC and the Advisory Committee on Immunization Practices (ACIP) on use of nirsevimab in young children. Infants and children recommended to receive nirsevimab should be immunized as quickly as possible. Healthcare providers should not reserve nirsevimab doses for infants born later in the season when RSV circulation and risk for exposure to RSV may be lower. RSV activity remains elevated nationwide and is continuing to increase in many parts of the country, though decreased activity has been observed in the Southeast.
|
|
Recommendations for Healthcare Providers
- In the setting of increasing supply, healthcare providers should administer a single dose of nirsevimab to all infants aged less than 8 months, as well as children aged 8 through 19 months at increased risk.
- Healthcare providers should continue to work with their state immunization program and the manufacturer to order available nirsevimab doses. CDC is working closely with jurisdictional partners to ensure adequate supply through the Vaccines for Children Program.
- Neither RSV vaccine (Pfizer Abrysvo, GSK Arexvy) is approved for use in infants or young children. Healthcare providers should take care to use the correct product for the correct population.
- Although supply of nirsevimab is expected to increase, available supply may continue to vary locally and by healthcare facility. For healthcare providers who continue to have limited supply, nirsevimab should be prioritized to protect infants at the highest risk for severe RSV disease using the following principles: first by high-risk conditions and then by age, prioritizing the youngest infants first.
-
Pregnant people 32 through 36 weeks gestation should receive RSV vaccination through January.
- Pfizer Abrysvo is the only RSV vaccine recommended for use in pregnant people. GSK Arexvy is not recommended for use in pregnant people.
- Administration of both nirsevimab and RSV vaccination for pregnant people is not needed to protect most infants.
|
COCA Now: January 22, 2024:
|
Information on Respiratory Syncytial Virus (RSV) Vaccine Administration Errors in Young Children and Pregnant People
|
|
Vaccine administration errors are known to occur and are routinely monitored through the Vaccine Adverse Event Reporting System1 (VAERS). Since approval of RSV vaccines and the monoclonal antibody nirsevimab, the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA) have received reports of the Pfizer (Abrysvo), or GSK (Arexvy) RSV vaccines being administered in error to young children. CDC and FDA have also received reports of the GSK RSV vaccine (Arexvy) being administered in error to pregnant people. As of January 17, 2024, the number of reports received by VAERS suggests that these types of errors are uncommon in young children less than 2 years of age (25 reports) and pregnant people (128 reports) relative to an estimated 1 million infants protected from RSV either through infant receipt of nirsevimab or through vaccination of pregnant people.2
In August and September 2023, CDC and the Advisory Committee on Immunization Practices recommended two RSV prevention products to prevent RSV-associated lower respiratory tract disease in infants. Nirsevimab (Beyfortus, Sanofi, and AstraZeneca) is only recommended for infants and some young children at increased risk for severe RSV disease. RSV vaccines (Pfizer Abrysvo, GSK Arexvy) are NOT approved for use in infants or young children. Pfizer (Abrysvo) is the only RSV vaccine recommended for pregnant people. The GSK RSV vaccine (Arexvy) is NOT approved for use during pregnancy.
Most reports of administration errors in young children occurred in infants younger than 8 months. Administration errors for both young children and pregnant people occurred in outpatient settings, including doctor’s offices; administration errors of the GSK RSV vaccine (Arexvy) in pregnant people also occurred in pharmacies. Most of these administration error reports described no adverse event. When an adverse event was concurrently reported to VAERS, most reports were classified as nonserious1. CDC, FDA, and other federal agencies continue to monitor the safety of RSV vaccines and reports of vaccine administration errors and will share information with the public as it becomes available.
|
|
Recommendations for Healthcare Providers who Have Administered Incorrect RSV Vaccine Products to Their Patients
- For infants and young children who are recommended to receive nirsevimab but received either the Pfizer (Abrysvo) or GSK (Arexvy) RSV vaccine in error, administer a dose of nirsevimab.
- For pregnant people who have received the GSK RSV vaccine (Arexvy) in error, do not give a dose of the Pfizer RSV vaccine (Abrysvo). Instead, the infant (if younger than 8 months) should receive nirsevimab during RSV season (October through March in most of the continental United States).
- Healthcare providers and facilities should ensure use of the correct RSV prevention product in the correct population and take actions to prevent vaccine administration errors, including automating error prevention alerts in electronic health record systems, ensuring proper education and training on vaccine recommendations, paying close attention to labeling, and following proper storage and administration best practices.
- Healthcare providers are strongly encouraged to report vaccine administration errors to VAERS.
- For questions about vaccine administration errors, healthcare providers can submit their questions to NIPINFO@cdc.gov.
- Healthcare providers in the United States with a complex vaccine safety question may request consultation on a vaccine administration error event for a specific patient. Information on how to request a consultation is available at the Clinical Immunization Safety Assessment (CISA) Project.
1 VAERS (managed by CDC and FDA) is a passive surveillance system that is used to detect possible vaccine safety problems and also monitors for vaccination errors. VAERS reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable and VAERS is not designed to determine if a vaccine caused a health problem. VAERS data are updated frequently and may change. VAERS reports that meet certain criteria are classified as serious.
2 Calculated using the National Immunization Survey Adult COVID Module (NIS-ACM) nirsevimab coverage data, Vaccine Safety Data link RSV maternal vaccination coverage data, and CDC Wonder birth data through December 2023. Several assumptions were applied (number of eligible persons, application of coverage estimates to eligible cohort, and no child-parent dyad receiving both immunizations).
Healthcare Provider Toolkit
RSV vaccination for pregnant people
RSV antibody immunization for infants
|
|
|
|
|
COCA Now: January 26, 2024:
|
Reminder of Recommendations for Seasonal Administration of Maternal RSV Vaccine
|
|
The Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP) recommend the RSV vaccination (Pfizer Abrysvo) for pregnant people during 32–36 weeks gestation using seasonal administration to protect infants against RSV-associated lower respiratory tract disease (LRTD) after birth. In most of the continental United States, the RSV vaccine should be given to pregnant people from September 1 through January 31, regardless of year-to-year circulation, when infants would be born during increased RSV activity, and the vaccination would provide the most benefits to the infant against RSV-associated LRTD after birth. Jurisdictions that have different RSV seasonality from most of the continental United States, such as Alaska, southern Florida, Guam, Hawaii, Puerto Rico, the U.S.-affiliated Pacific Islands, and the U.S. Virgin Islands, may consider RSV vaccination of pregnant people after January 31. Infants born to unvaccinated mothers should receive nirsevimab, a long-acting monoclonal antibody that provides immediate protection to the infant against RSV-associated LRTD.
|
Recommendations for Healthcare Providers on the Seasonal Administration of the RSV Vaccine (Pfizer Abrysvo)
- In most of the continental United States, administer the maternal RSV vaccine (Pfizer Abrysvo) from September 1 through January 31.
- Healthcare providers who administer the RSV vaccine to pregnant people after January 31 should encourage patients to check with their insurance plans on coverage details, as coverage and cost-sharing by private insurance plans may vary after January 31. Providers should consider submitting an insurance test claim to estimate out-of-pocket costs.
- In jurisdictions where seasonality differs from most of the continental United States, such as Alaska, southern Florida, Guam, Hawaii, Puerto Rico, the U.S.affiliated Pacific Islands, and the U.S. Virgin Islands, healthcare providers should follow state, local, or territorial guidance on timing of administering the RSV vaccine (Pfizer Abrysvo) for pregnant people.
- CDC recommends protecting all infants against RSV-associated LRTD through either the RSV vaccine for pregnant people (Pfizer Abrysvo) or infant receipt of nirsevimab. Administration of both products is not needed for most infants.
- For infants age less than 8 months born to unvaccinated mothers, healthcare providers should administer nirsevimab from October 1 through March 31; however, healthcare providers can administer nirsevimab outside of this time frame based on local epidemiology
|
For any questions, please contact the Maine Immunization Program at (207) 287-3746 or email ImmunizeME.DHHS@maine.gov
|
|
|

