2026 Kansas Immunization Conference
Pre-Conference: May 19
General Session: May 20
Wichita Marriott
Mark your calendars for the 2026 Kansas Immunization Conference.
Call for Nominations!
We are searching for the next Kansas Immunization Champion and need help. If you know someone in your community who is fostering immunizations, please help us honor and recognize their efforts!
The Immunization Champion Award recognizes individuals who are working at the local level and is hosted by the Association of Immunization Managers (AIM). The national award honors those doing an exemplary job or going above and beyond to promote or foster immunization in their community for children and adults.
Anyone can nominate an Immunization Champion. Champions are selected by their local or state immunization programs, who evaluate nominees by the following criteria: leadership, collaboration, innovation, and/or advocacy. Learn more about this prestigious award and access the nomination form here.
Nominations must be submitted by June 4, 2026, and the champion will be notified in early August.
Champion Eligibility:
Individuals can be recognized for their work in childhood, adolescent, or adult vaccinations.
Who is eligible?
- Health care professionals (i.e., pharmacists, physicians, nurses, physician assistants, nurse practitioners, medical assistants)
- Nonprofit leaders
- Community activists
- Parents
- School and education leaders
- Coalition members
- Community-based organization members
- Immunization partners
For a list of complete ineligibility criteria, review the ineligibility section of the nomination form here.
If you have any questions or to submit nominations, please contact Krissi O’Dell, Immunization Nurse Educator, via email at Krissi.odell@ks.gov.
Additional information can also be found at Immunization Champion Awards - Association of Immunization Managers.
Annual recertification for Vaccines for Children (VFC) and Vaccines for Adults (VFA) providers will be opening soon. Recertification is completed electronically in KSWebIZ by the primary or backup VFC/VFA contact, or by the physician/medical director.
During recertification, providers will review clinic staff information, update the number of patients served by the facility, review program requirements, and complete the provider agreement.
Recertification dates will be announced soon.
What can providers do now?
To help make the recertification process as smooth as possible, providers are encouraged to complete a few steps in advance.
Review contact information. Verify that the medical director, primary contact, backup contact, and secondary contact information in KSWebIZ is current and accurate.
Confirm physician contacts. Make sure all prescribing staff are listed as physician contacts in KSWebIZ and that their information is correct.
Taking these steps now can help reduce delays and make annual recertification quicker and easier once it opens.
If you have questions, please contact your Regional Immunization Nurse or Nurse On-Call at 877-296-0464.
Influenza activity in Kansas continues to steadily decline from peak activity identified in late December; however, activity remains elevated. During the week ending March 14, 2026, 3.9% of visits reported by participating Influenza-Like Illness Surveillance Network (ILINet) providers were due to influenza-like illness (ILI), defined as fever (≥100°F) with cough and/or sore throat (Figure 1). Emergency department discharge data captured through syndromic surveillance indicated that 3.9% of emergency department visits in Kansas were associated with ILI (Figure 2).
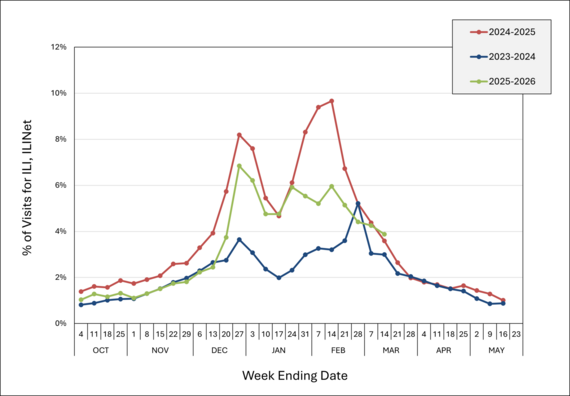 Figure 1. Percentage of Visits for ILI Reported by ILINet Sites, Kansas, October 2025 – Present
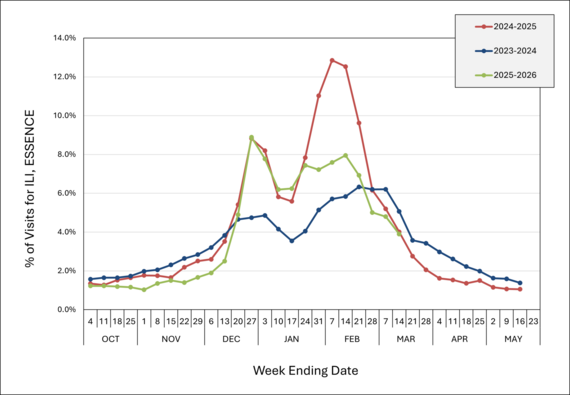 Figure 2. Percentage of ED Visits for ILI Reported to ESSENCE, Kansas, October 2025 – Present
During the week ending March 14, 2026, the Kansas Health and Environment Laboratories (KHEL) detected influenza in one specimen. This specimen was positive for influenza A(H3). Influenza A(H3) remains the predominant strain detected among specimens submitted by Kansas facilities. Wastewater surveillance data from participating sites in three Kansas counties indicates that currently, influenza A levels are low and influenza B levels are high.
As of March 18, 2026, there were four active influenza outbreaks across the state. A total of 110 influenza outbreaks have been reported during the 2025-2026 season so far. Outbreaks of influenza and other reportable diseases should be reported to the KDHE Epidemiology Hotline at (877) 427-7317 within four hours of suspicion.
Resources:
Summary
In the continental United States, the recommended seasonal time frame for administration of RSV monoclonal antibodies typically starts in October and continues through March 31, with flexibility for public health authorities to adjust timing based on local RSV activity.
The RSV monoclonal antibodies nirsevimab (Beyfortus) and clesrovimab (Enflonsia) are recommended for all infants < 8 months born during or entering their first RSV season (who were not protected by maternal RSV vaccination during pregnancy), and nirsevimab is recommended for high-risk children 8–19 months entering their second RSV season.
RSV activity started late in Kansas this season, which suggests the risk of RSV infection may continue longer than usual into the spring.
Providers should extend the recommended timeframe for administration of nirsevimab and clesrovimab to eligible infants and young children for the prevention of severe RSV disease through April 30, 2026. Providers should use clinical judgment to weigh current and future risk of severe RSV disease, knowing that receipt of RSV monoclonal antibody at the end of the 2025-2026 season will preclude receipt of another dose at the beginning of the 2026-2027 season, except for high-risk children.
All other guidance for RSV infant monoclonal antibody administration remains unchanged at this time. KDHE will continue to monitor RSV activity in Kansas and will communicate additional information as needed.
Background
RSV monoclonal antibodies are typically recommended to be administered to eligible infants each RSV season from October 1 through March 31 in the continental U.S., with allowance for administration outside this time frame in tropical locations and Alaska, or in the setting of increased RSV activity outside typical months.
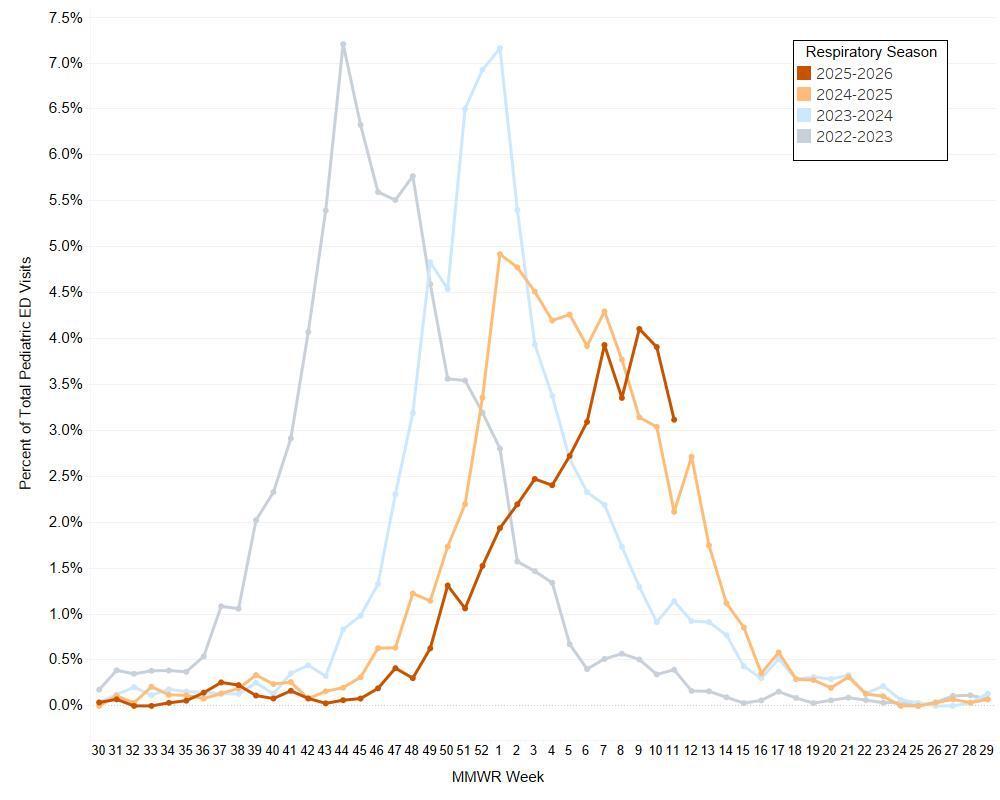
RSV activity in Kansas in the current 2025-2026 season began later than in recent past seasons, and RSV activity continues to be high (Figure 1). In the previous three seasons, RSV activity began increasing in September, October, and November, respectively, with peaks occurring within approximately a month before activity began to decline. In the current season, activity began increasing steadily in December 2025 (MMWR week 49), reached high levels and peaked at the end of February and into March (MMWR weeks 6–11). While some epidemiological metrics indicate that RSV activity may be declining, the duration and intensity of the remaining RSV season is currently unknown. Given the high risk of severe RSV disease among newborns and young infants, immunizing providers in Kansas should consider RSV monoclonal antibody administration through April 30, 2026. KDHE will continue to monitor RSV activity in Kansas and will communicate additional information as needed.
Figure 1. Weekly Percentage of Kansas Emergency Department Visits for Respiratory Syncytial Virus (RSV) Among Pediatric Visits (Patients < 13 Years)
 Data Source: Kansas Department of Health and Environment, Kansas Syndromic Surveillance Program.
RSV Monoclonal Antibody Recommendations
Infants < 8 months: Administer one dose to infants born during or entering their first RSV season who are not protected already by maternal RSV vaccination during pregnancy.
- Nirsevimab: 50 mg for infants < 5 kg; 100 mg for infants ≥ 5 kg or
- Clesrovimab: 105 mg regardless of weight
Children (8–19 months): Children entering their second RSV season who are at increased risk for severe disease (e.g., chronic lung disease of prematurity, severe immunocompromise, or cystic fibrosis) and American Indian and Alaska Native children should receive nirsevimab.
- Nirsevimab: 200 mg (administered as two 100 mg injections)
Considerations for Clinicians
Providers should use clinical judgment to weigh current risk factors for severe RSV disease in the time that remains in the 2025-2026 season, including age and potential for exposure to RSV, against the future risk of severe RSV disease in the upcoming 2026-2027 season when deciding whether to immunize an eligible infant with nirsevimab or clesrovimab from April 1-30, 2026.
Receipt of RSV monoclonal antibody at the end of the 2025-2026 season will preclude receipt of another dose at the beginning of the 2026-2027 season, unless the child has risk factors that would make them eligible for a dose in their second RSV season.
RSV monoclonal antibodies can be administered simultaneously with other age-appropriate vaccines, including hepatitis B, influenza, and COVID-19.
In Kansas, recommended maternal RSV vaccination during pregnancy ended January 31, 2026. This administration window is not being extended.
For more information:
|

