 A study conducted in two rural Massachusetts jails found that people with opioid use disorder who were incarcerated and received buprenorphine, a medication approved to treat opioid use disorder, were less likely to be arrested or convicted again after release than those who did not receive the medication. After adjusting the data to account for baseline characteristics, such as prior history with the criminal justice system, the study revealed a 32% reduction in rates of probation violations, reincarcerations or court charges when the facility offered buprenorphine to people in jail compared to when it did not. The findings were published in Drug and Alcohol Dependence.
The study was conducted by the Justice Community Opioid Innovation Network (JCOIN), a program to increase high-quality care for people with opioid misuse and opioid use disorder in justice settings and funded by the National Institute on Drug Abuse (NIDA), part of the National Institutes of Health, through the Helping to End Addiction Long-term Initiative or NIH HEAL Initiative.
“Studies like this provide much-needed evidence and momentum for jails and prisons to better enable the treatment, education, and support systems that individuals with an opioid use disorder need to help them recover and prevent reincarceration,” said Nora D. Volkow, M.D., NIDA Director. “Not offering treatment to people with opioid use disorder in jails and prisons can have devastating consequences, including a return to use and heighted risk of overdose and death after release.”
A growing body of evidence suggests that medications used to treat opioid use disorder, including buprenorphine, methadone, and naltrexone, hold great potential to improve outcomes among individuals after they’re released. However, offering these evidence-based treatments to people with opioid use disorder who pass through the justice system is not currently standard-of-care in U.S. jails and prisons, and most jails that do offer them are in large urban centers
 Increased opioid use in Ohio is believed to have contributed to a crisis within county child welfare agencies throughout the state. Prior research has found a connection between opioid use and child abuse and neglect, but no previous studies have examined the relationship between opioid overdoses and child maltreatment rates at a neighborhood level. The sample is 9,231 U.S. Census block groups in Ohio for 2015. Bayesian conditionally autoregressive models were used to examine the relationship between naloxone administrations (as a proxy for overdose) and child maltreatment.
The study controlled for variables representing social disorganization characteristics including unemployment, racial/ethnic heterogeneity, and vacant housing rates. It specifically examined child maltreatment referrals per child population and child maltreatment substantiations per child population. Higher rates of naloxone administration by emergency medical services were related to higher rates of referrals for child welfare investigations (relative risk = 1.0026) and substantiations (relative risk = 1.0027) at the block group level. Neighborhoods located in Appalachia with higher rates of overdoses were at greater risk for experiencing more referrals for child welfare investigations (relative risk = 1.0043).
As communities continue to struggle with containing opioid misuse and reducing opioid overdose deaths, they must also contend with addressing problems that may arise from overdoses, including child abuse and neglect. The findings suggest that the relationship between overdoses and maltreatment occurs at a much smaller spatial scale that has previously been observed. This may allow resources to be targeted more effectively within counties and communities.
More information can be found by viewing the original study.
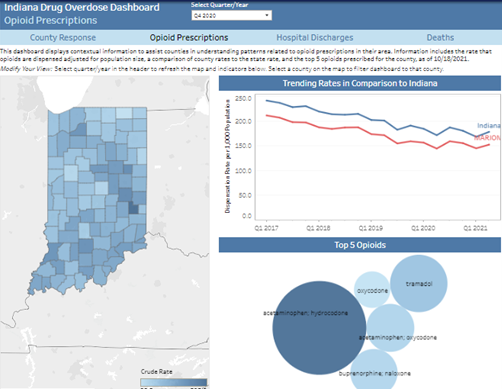 Please visit the Indiana Drug Overdose Dashboard, where you will find data from 2017 up to provisional data for 2021. In this dashboard, you will find data regarding opioid prescriptions, hospital discharges, and drug-related deaths.
|


