|
These include peer review, credentialing and privileging, and quality and patient safety monitoring. The organized medical staff has also historically served as a professional forum and communication network for physicians to discuss clinical issues and address professional concerns. Within certain structures, the medical staff allows the sharing of information in a safe, confidential, and legally protected space.
 |
Notably, under the Health Care Quality Improvement Act of 1986, professional review activities are legally protected, though it is incumbent on organized medical staffs to report to their state board any “professional review action that adversely affects the clinical privileges of a physician for a period longer than 30 days” or “accepts the surrender of clinical privileges of a physician while the physician is under an investigation by the entity relating to possible incompetence or improper professional conduct, or in return for not conducting such an investigation or proceeding.”4
At its best, the organized medical staff provides robust, well-validated mechanisms to ensure that patients are protected from avoidable harm and that poor care is remediated or, as a last resort, results in expulsion from the organized medical staff, with attendant loss of privileges to practice. However, there are risks to the organized medical staff model that must be recognized and managed with intentionality and due caution. Significantly, the historical culture of the organized medical staff model could in some instances be susceptible to professional protectionism against outside criticism or accountability. Although the “Minimum Standard” created a huge step forward in accountability to physician colleagues rather than solely oneself, the idea of accountability to other stakeholders was often met with resistance. Resistance to broader accountability could then prove a potential barrier to quality and patient safety efforts tied to standardizing care around widely accepted evidence-based medicine frameworks.3
In contrast, those healthcare organizations (and by extension, their organized medical staffs) that embrace interdependence, objective standards of care, and accountability of all clinical staff to key stakeholders (including non-physician licensed professionals, regulators, patients and patient advocates, and community board members) will have the advantage in achieving the best and safest medical care for our patients.4 In particular, having non-physician stakeholder voices, including PAs and NPs, on key committees of the organized medical staff is increasingly viewed as best practice. CMS Conditions of Participation now explicitly allow NPs, PAs, CRNAs, and midwives to be full members of organized medical staffs (at the discretion of the organized medical staff and as allowed by state law).2
In the State of Idaho, the organized medical staff is also responsible for the oversight of physician assistants (PAs) in their practice of medicine within facilities governed by an organized medical staff. Per Idaho Code Idaho Code 54-1807A “The degree and nature of collaboration shall be determined by the facility or practice in which the physician assistant works and shall be set forth in facility bylaws or procedures for facilities that have credentialing and privileging systems […] Such provisions may provide for collaborative oversight to be provided by the employer, group, hospital service, or the credentialing and privileging systems of a licensed facility, but at a minimum shall require a physician assistant to collaborate with one (1) or more physicians licensed pursuant to this chapter. Such physicians need not be identified individually in the facility bylaws or procedures or collaborative practice agreement if more than one (1) physician works in the facility or practice.” Idaho law recognizes the robust oversight functions inherent in credentialing, privileging, and peer review provided by the organized medical staff framework, and for PAs practicing within organized medical staff structures, allows for these collective functions to ensure safe care rather than individualized collaborative practice agreements.5 Although not legally required under the Health Care Quality Improvement Act of 1986, organized medical staffs may report professional review action that adversely affects the clinical privileges for a “health care practitioner who is not a physician, if the entity would be required to report such information […] if the practitioner were a physician.”4
For those physicians and PAs who serve their organized medical staff, and by extension, our hospitals, communities, and patients, the Idaho Board of Medicine offers sincere gratitude for your commitment to this vital function of our healthcare system.
References:
1. American College of Surgeons ACS Archives: The “Minimum Standard” document https://www.facs.org/about-acs/archives/past-highlights/minimumhighlight/
2. MEDICARE CONDITIONS OF PARTICIPATION §482.12(a) Standard: Medical Staff Medicare_COP_Summary_12-2020.pdf
3.Redesign the Medical Staff Model: A Guide to Collaborative Change (ACHE Management Series) by Jon Borroughs, MD, Health Administration Press, 2015
4. Health Care Quality Improvement Act of 1986 H.R.5540 - 99th Congress (1985-1986): Health Care Quality Improvement Act of 1986 | Congress.gov | Library of Congress
5. Idaho Code 51-1807A Idaho Code 54-1807A – Physician Assistants — Physician Assistant Advisory Committee » LawServer
2026 Summary of Passed Legislation
Agency Sponsored Legislation:
The Idaho Board of Medicine is providing an overview of several regulatory changes resulting from legislation passed during the 2026 legislative session. Licensees are encouraged to review each bill in its entirety, along with any other pertinent legislation not listed below, and assess the impact these changes may have on their practice.
House Bill 703 – Universal Discipline Procedure:
During the 2026 legislative session, many bills passed that impacted the Division of Occupational and Professional Licenses’ (DOPL) work. Among those was HB703, known as “Universal Discipline”. This bill, which takes effect July 1, 2026, accomplishes three main objectives:
- Simplifies and removes repetitive or inconsistent language across practice acts regarding discipline.
- Provides a new section of code which identifies standardized, consistent due process protections for licensees. It also creates a baseline set of consequences when a board chooses to act.
- Defines DOPL’s role and responsibilities throughout the disciplinary process.
The standardized language also supports uniform processes for the investigation, communication, and processing of discipline cases across the division, found in Idaho Code § 67-2616. While the new law does lower the Board of Medicine’s administrative fine cap to a maximum of $1,000 per offense, the Division and Board can now seek a civil judgment against a licensee who created financial loss for a member of the public. Another new provision allows complainants to receive updates regarding the status of a filed complaint, upon request. “This legislation benefits licensees and boards by replacing roughly one hundred scattered, duplicative disciplinary procedures with one clear and consistent process,” said Kolby Reddish, DOPL Deputy Administrator. “This makes expectations easier to understand, proceedings easier to navigate, and outcomes more predictable across all Division boards."
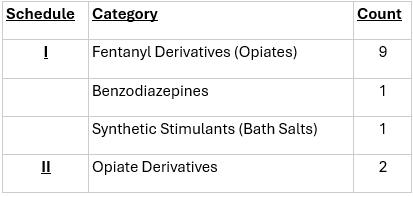
House Bill 777 – Uniform Controlled Substances:
The Division of Occupational and Professional Licenses (DOPL), on behalf of the Idaho Board of Pharmacy, provides an annual update to the Legislature on necessary changes to the Uniform Controlled Substances Act found in Title 37, Chapter 27 of Idaho Code. Thirteen (13) substances were scheduled as a result of this legislation: eleven (11) were added to Schedule I, and two (2) were added to Schedule II. The additions to Schedule II are not new; rather, they were inadvertently excluded from past controlled substance updates. Each scheduling decision was independently reviewed by the Board and made according to the risk associated with its prescriptive use. Technical corrections were incorporated to align administrative implementation with clearer statutory language. Access to the Idaho Prescription Drug Monitoring Program (PDMP) was expanded to permit federal entities, such as the U.S. Department of Veterans Affairs or Indian Health Service, to use it in the normal course of patient treatment and monitoring of inappropriate controlled substance prescribing. These changes go into effect on July 1, 2026.
 |
House Bill 787 – Podiatric Medical Practice Act
In alignment with the Governor’s Executive Order 2025-05, which sought to increase governmental efficiency, the Division brought forward this bill to consolidate the Board of Podiatry into the Board of Medicine. To accommodate this change, the composition of the Board of Medicine was amended to include a licensed podiatrist and remove the position previously allocated for the Director of the Idaho State Police. The rule chapter governing podiatry was also repealed and its provisions shifted into statute. This reflects an emerging legislative priority to move shorter rule chapters into statute. The effective date of the bill is July 1, 2026.
Non-Agency Legislation:
House Bill 491 – Emergency Mental Health First Aid
Effective July 1, 2026, this bill amends Idaho’s Good Samaritan law to extend liability protections to any individual who, in good faith and without compensation, provides emergency psychological assistance during a mental health or suicidal crisis.
Senate Bill 1294
This bill creates Section 39-905A of Idaho Code, requiring infants and newborns to receive a hearing screening prior to discharge from a hospital, health care facility, or birthing facility. For births occurring outside of those settings, the birthing attendant is required to ensure the infant or newborn is screened or referred for screening within twenty-one (21) days of birth. The bill also establishes approved screening methods, reporting requirements for failed screenings, and monthly reporting requirements for other screening results. Finally, enforcement of the bill is contingent on continued federal funding or, in the event federal funding is lost, a determination that administration would not increase costs to the state. The bill will become effective on July 1, 2026.
Senate Bill 1316
In relation to Senate Bill 1294, this bill allows a parent or guardian to claim an exemption from any screening tests for a child if the parent or guardian:
- Objects on religious or other grounds, including philosophical or conscientious beliefs; or
- Submits a certificate signed by a physician licensed by the state Board of Medicine stating that the child’s physical condition is such that any or all of the requirements would endanger the life or health of the child.
The bill will become effective on July 1, 2026.
Controlled Substance Dispensation Reporting Reminders
Timing of Dispensation Reporting:
As of 07/01/2025, Idaho Statute 37-2730A requires drug outlets dispensing controlled substances in or into Idaho to report controlled substance dispensing by the end of the business day, replacing the previous next-business-day deadline. The board's policy permits an exception for emergency room dispensing reported by a drug outlet, allowing submission the following day. The adherence to this requirement has been slow or incomplete. Drug outlets that have been unable to adhere to this requirement should consider altering their procedures to ensure compliance with current law.
Dispensation Report field DSP17 – Date Sold:
DSP17 - The ‘Date Sold’ field was deemed a required entry for Idaho PDMP dispensation reports in 11/2021. Recently, it was discovered that the field entry requirement was unintentionally lifted. To correct this, the PDMP clearinghouse will soon issue soft warnings before requiring re-entry into the field. It is advisable to proactively begin entering the sold date, if applicable, to ensure your vendor is informed. Thank you for helping make this transition smooth.
If you have questions regarding the PDMP, please contact Wendy Muir, Program Information Coordinator, Idaho Prescription Drug Monitoring Program, at 208-817-6195.
|