|
Welcome to the bimonthly bulletin for the Bureau of HIV, STD & Hepatitis. If you would like to include items, or have suggestions on how to improve the usefulness of the bulletin, please submit them to any of the program staff.
The staff directory is located here.
In December, IDPH will be participating in a meeting with the Center for Disease Analysis and several stakeholders to develop a hepatitis C elimination model for Iowa. This project was a result of IDPH’s work on the development of the hepatitis C epidemiological profile, developed with a grant from the Association of State and Territorial Health Officials (ASTHO). Several variables will be considered, including access to treatment.
Recently, the National Viral Hepatitis Roundtable and the Harvard Center for Health Law and Policy Innovation assessed the state of access to hepatitis C (HCV) treatment for Medicaid enrollees in every state. They developed report cards for each state with an in-depth evaluation of the most significant restrictions to treatment, including liver damage restrictions sobriety restrictions, and prescriber restrictions. Iowa received a score of “D” because of “severe restrictions in all categories.” The model may give us some information on how these restrictions affect the state’s ability to eliminate hepatitis C. Stay tuned for more information on the HCV elimination model!
Reported cases of gonorrhea are increasing quickly in Iowa. By mid-October 2017, the number of cases reported had already exceeded the 2,600 gonorrhea cases reported in 2016. We estimate there will be over 3,400 gonorrhea diagnoses reported by the end of 2017. This would be a 131 percent increase since 2013.
Gonorrhea is increasing throughout the U.S. Indiana, for example, reported exceeding their entire number of 2016 cases by October of this year. Gonorrhea increased by nearly 19 percent in the U.S. from 2015 to 2016.
There are likely many reasons for the increases. For one, more providers are conducting oropharyngeal and rectal testing, which has identified infections that may have otherwise been missed in the past. However, these steep increases most likely indicate increased transmission, as well. Furthermore, while the increases are occurring in both women and men, recent trends indicate the rate of increase is higher among men. This likely signals an increase among men who have sex with men.
Decreasing the time between infection and treatment is a key strategy in combating gonorrhea. This can be accomplished by increasing testing to ensure that infected individuals are diagnosed and given adequate treatment. Adherence to the CDC STD Treatment Guidelines (250mg ceftriaxone plus 1 gram azithromycin) is essential given the speed at which Neisseria gonorrhoeae develops drug resistance. For more information on gonorrhea, please contact George Walton.
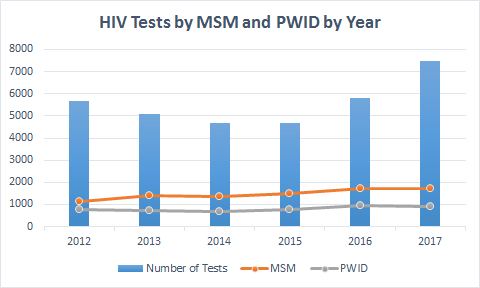
Kudos to all IDPH-funded HIV and hepatitis test sites! You have increased services significantly in 2017. Data are presented below.
HIV Testing:
- As of October 31, 7,469 tests were administered, compared to 4,616 at the same time in 2016
- 27 individuals (0.36%) tested positive for HIV
- 85% of newly identified HIV-positive clients attended their first medical appointment within 90 days of diagnosis
- 25% of individuals tested for HIV identified as MSM or MSM/IDU and 12% of individuals were persons who inject drugs (PWID)
- 33% of individuals tested for HIV identified as black/African American or Latino
MSM: Men who have sex with Men || PWID: People who inject drugs
Hepatitis C Testing
As of October 31, 2017, 1,792 tests were administered, compared to 518 at the same time in 2016
- 80 (4%) individuals were identified as antibody positive for hepatitis C
- Of those individuals who had an antibody positive test, 43 (54%) were RNA positive (marker for chronic infection)
- 31% of individuals tested for HCV were ages 20 to 39 (90% reported injection drug use)
- 58% of individuals tested for HCV were baby boomers (born between 1945 and 1965)
Hepatitis A/B Immunizations
- 440 combination hepatitis A/B vaccinations were administered
The Iowa Department of Public Health’s (IDPH) Quality Improvement (QI) Council is charged with leading QI activities within IDPH. The RW Part B Program will be partnering with the HIV Surveillance Office to participate in a QI activity to improve the viral load and CD4+ cell count lab-import process.
We know how essential lab results in CAREWare are to case managers, and how frustrating it can be when results are missing from the system. We’ve discovered some kinks in the process and are determined to fix them!
The IDPH QI Coordinator and an IDPH QI Council member will be facilitating the one-day event. The goals of the event are to improve the sharing of lab results between the HIV Surveillance Office and the RW Part B Program to reduce the number of errors in the importing process, and to reduce the frequency of missing results in CAREWare.
We will be flowcharting the entire process, starting with a case manager submitting a Case Management Enrollment and Client Consent Form, and ending with the successful and accurate lab import into CAREWare. A case manager will also be attending the event to bring her perspective on the process and to provide suggestions for improvements. The event will be held Friday, December 8. We look forward to sharing the improvements we make to the process!
IDPH partners with the Iowa Primary Care Association to increase HIV, HCV and STD routine testing at the 14 Federally Qualified Health Centers (FQHCs) in Iowa. There are 10 FQHCs participating in the routine screening project. One FQHC is in the implementation phase of the project.
Two out of the four FQHCs not participating in the project already provide testing in some capacity. One of the FQHCs is a migrant health program that faces significant barriers that make screening, follow up and treatment of patients quite difficult.
The purpose of this testing project is to increase testing among Iowans who may not otherwise receive it, and to facilitate linkage to care and treatment. USPSTF guidelines for testing of HIV, STD, and HCV are promoted at the FQHCs. Opt-out HIV testing is administered to all individuals between 13 and 65 years of age who have not been screened previously. All sexually active individuals under the age of 25 are screened annually for STDs. All individuals who are baby boomers (born between 1945 and 1965) who have not been screened previously for HCV.
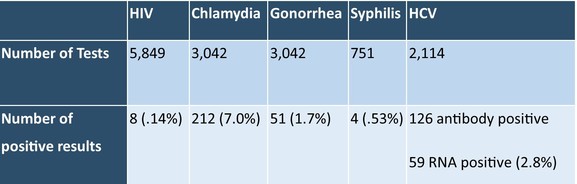
2017 Year-to-Date Screening Data:
Due to the high number of individuals testing positive for hepatitis C in southeastern Iowa, a partnership was launched between Community Health Centers of Southeastern Iowa and the University of Iowa Hospitals and Clinics to provide consultation on treating patients diagnosed with hepatitis C. This allows the health center patients to be treated for HCV on site at the community health center rather than traveling to Iowa City, which can be a burden. This consultation project with UIHC will be expanded in the future to include Promise Community Health Center in Sioux Center.
- George Walton, STD Program Manager, has been named to the board of the National Coalition of STD Directors. Congratulations George!

|