COVID-19 Alaska Clinical Update – June 13
Monday, June 13
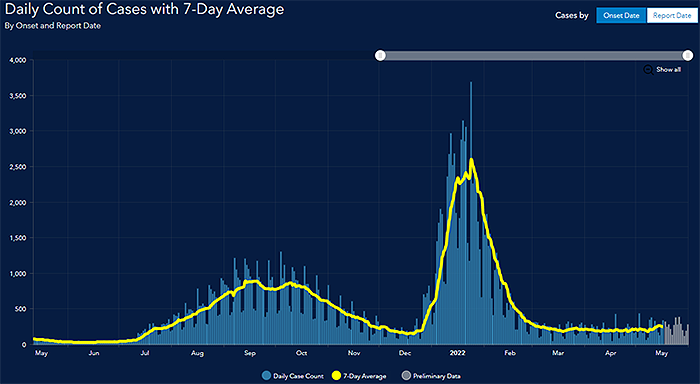
Graph taken from State of Alaska’s COVID-19 Cases Dashboard
Articles summarized in this update are compiled from a variety of sources but draw heavily on updates and resources highlighted in the Johns Hopkins Center for Health Security’s weekly COVID-19 update.
FDA schedules meeting for June 14-15 to review data on COVID vaccines for children 6 months to 5 years
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) is scheduled to meet on June 14-15 to discuss updates to the Moderna and Pfizer-BioNTech EUAs for their COVID-19 vaccines to include children 6 years and younger. In late April, Moderna submitted an EUA request to the FDA for its COVID-19 vaccine for children age 6 months to 6 months. Pfizer-BioNTech, which revised its study protocol for children 6 months to 5 years to include a third vaccine dose after two doses didn’t generate an adequate immune response, completed its EUA request on June 1 for its three-dose regimen.
The most recent data released on May 23 by Pfizer-BioNTech on their study of vaccine efficacy in children 6 months to 5 years shows that three doses of the mRNA vaccine were 80.3% effective at preventing infection among children when the Omicron variant was predominant. These data are based on only 10 cases diagnosed among the 1,678 study participants by the end of April, a number lower than the study’s 21-case threshold for analysis.
Pfizer-BioNTech COVID-19 booster vaccination authorized for children age 5 through 11 years
On May 19, the CDC’s Advisory Committee on Immunization Practices (ACIP) recommended that all children ages 5 to 11 should receive a Pfizer-BioNTech booster, or third, shot 5 months after completing the 2-dose primary series with the same vaccine, the only one currently authorized for use among that age group. The announcement also noted that more than 4.8 million children in this age group have been diagnosed with COVID-19, 15,000 have been hospitalized, and at least 180 have died of the disease.
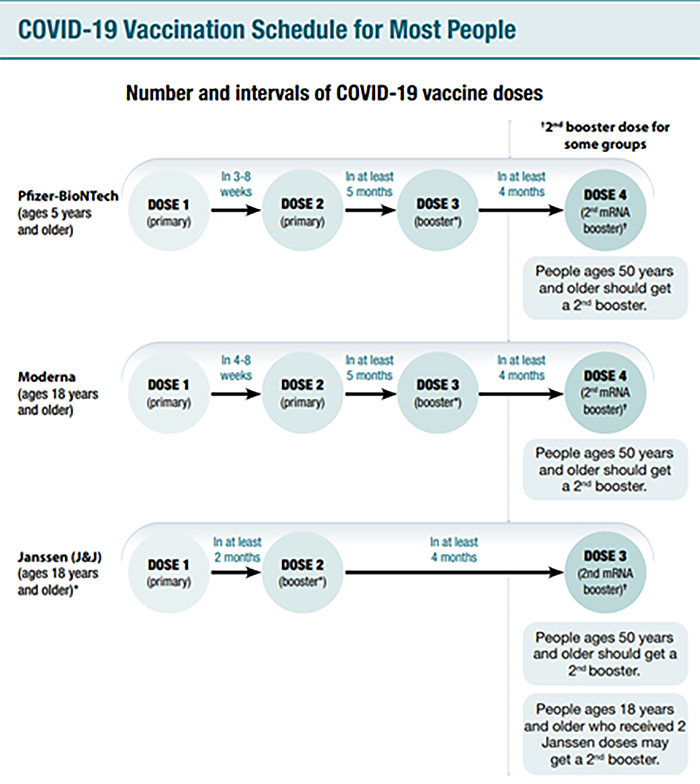
COVID-19 Vaccination Schedules
FDA advisory committee recommends approval of Novavax COVID-19 vaccine
On June 7, the FDA’s Vaccine and Related Biological Products Advisory Committee recommended FDA approval for the Novavax COVID-19 vaccine. The Novavax vaccine contains nanoparticles made up of proteins from the surface of the coronavirus, a fundamentally different design than the three shots currently available in the United States. The Novavax vaccine has been authorized in dozens of countries and has also received clearance from the European Union and World Health Organization. In clinical trials, the Novavax vaccine was found to have an efficacy of 90.4 percent at preventing mild, moderate or severe infection with older variants of the virus. None of the volunteers who got the vaccine experienced moderate or severe infection, translating to an efficacy of 100 percent. Although the FDA VRBAC committee voted to recommend the vaccine, due to recent manufacturing process changes by Novavax, the FDA needs to review further before deciding whether to authorize the vaccine.
Monkeypox
No cases of monkeypox have been detected in Alaska as of June 7, 2022. The Division of Public Health has published an information page on monkeypox with education for healthcare professionals and FAQs. Health care providers in Alaska should report suspected monkeypox cases to SOE immediately; please call SOE at 907-269-8000, or 1-800-478-0084 after hours. SOE can assist providers in obtaining appropriate clinical specimens that should be routed to the Alaska State Public Health Laboratory (ASPHL) in Anchorage for testing.
- The rash associated with monkeypox involves vesicles or pustules that are deep-seated, firm or hard, and well-circumscribed; the lesions may umbilicate or become confluent and progress over time to scabs.
- Presenting symptoms typically include fever, chills, the distinctive rash, or new lymphadenopathy; however, onset of perianal or genital lesions in the absence of subjective fever has been reported.
- The rash associated with monkeypox can be confused with other diseases that are encountered in clinical practice (e.g., secondary syphilis, herpes, chancroid, and varicella zoster). However, a high index of suspicion for monkeypox is warranted when evaluating people with a characteristic rash, particularly for men who report sexual contact with other men and who present with lesions in the genital/perianal area or for individuals reporting a significant travel history in the month before illness onset or contact with a suspected or confirmed case of monkeypox.
Additional information and pictures can be found on the CDC website for Monkeypox Signs and Symptoms

Remdesivir approved for treatment of COVID-19 in children 28 days and older who are either hospitalized or not hospitalized but have mild-moderate COVID-19 and are at high risk for progression to severe COVID-19
On April 25, the FDA expanded the approval of the COVID-19 treatment Veklury (remdesivir) to include pediatric patients 28 days of age and older weighing at least 3 kilograms (about 7 pounds) with positive results of direct SARS-CoV-2 viral testing who are hospitalized or not hospitalized but have mild-to-moderate COVID-19 and are at high risk for progression to severe COVID-19, including hospitalization or death. While remdesivir had been available to this population previously under an EUA, it is now the first approved COVID-19 treatment for children less than 12 years of age.
BA.4/BA.5 Subvariants
From Johns Hopkins Center for Health Security COVID-19 Update: On May 12, the European Centre for Disease Prevention and Control (ECDC) reclassified the Omicron BA.4 and BA.5 sublineages from variants of interest to variants of concern (VOC). BA.4 and BA.5 were first identified in South Africa in January and February 2022, respectively. Similar to other Omicron subvariants, such as BA.2, BA.4 and BA.5 appear to be significantly more transmissible than previous variants. BA.5 has an estimated growth advantage of 13% over BA.2 under laboratory conditions. Even individuals previously infected with an Omicron variant do not appear to be well protected against infection from BA.4/BA.5. Notably, BA.4/BA.5 contain enough mutations in key sites to evade both naturally acquired immunity and previous vaccinations. Fortunately, BA.4 and BA.5 do not appear to cause more severe disease than previous variants, although more studies are needed to solidify this observation. In the US, BA.2 and BA.2.12.1 still remain the dominant subvariants at this time, but it is likely that more cases will result from BA.4/BA.5 infection as the summer approaches and as more cases are imported from South Africa and Europe.
NIH Treatment Guidelines Updates
The NIH updated its COVID-19 Treatment Guidelines on May 31. The updates include 4 new sections discussing the care of children critically ill with COVID-19 or multisystem inflammatory syndrome in children (MIS-C); new information informing treatments to prevent blood clots among patients with COVID-19; additional rationale in sections discussing critical care for adults with COVID-19; new information about the use of Evusheld (tixagevimab/cilgavimab) for pre-exposure prophylaxis among immunocompromised individuals; and other information.
Alaska Public Health Alert - Shortage of Iodinated Contrast
The COVID-19 lockdown in Shanghai temporarily closed the main factory that manufactures iodinated contrast used in CT studies. Although production has resumed, there is a global shortage of contrast that is expected to last through June 2022. On June 9, there was an Alaska Public Health Alert on the Shortage of Iodinated Contrast. Key takeaways include “Clinicians should consider if contrast is necessary for a desired imaging study and consider if an alternative test of equal clinical utility could be used. If in doubt, consult your radiologist. Clinicians should NOT delay a patient’s diagnostic testing or procedures secondary to the current shortage at this time.” In addition, hospitals and outpatient diagnostic centers should establishing mitigation and allocation strategies. The American College of Radiology has offered temporary guidance for alternative imaging and risk mitigation strategies.
CDC Health Advisory addresses risk of “COVID-19 rebound” after Paxlovid treatment
On May 24, the CDC released a Health Advisory to update healthcare providers, public health departments, and the public about the potential for recurrence of COVID-19 or “COVID-19 rebound.” COVID-19 rebound has been reported to occur between 2 and 8 days after initial recovery and is characterized by a recurrence of COVID-19 symptoms or a new positive viral test after having tested negative. A brief return of symptoms may be part of the natural history of SARS-CoV-2 infection in some persons, independent of treatment with Paxlovid and regardless of vaccination status. Limited information suggests that persons treated with Paxlovid who experience COVID-19 rebound have had mild illness; there are no reports of severe disease. There is currently no evidence that additional treatment is needed with Paxlovid or other anti-SARS-CoV-2 therapies in cases where COVID-19 rebound is suspected.
FDA approves baricitinib for treatment of COVID-19 in hospitalized patients
On May 10, the FDA approved a Olumiant (baricitinib) for the treatment of COVID-19 in hospitalized adults requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or ECMO. Olumiant is the first immunomodulatory treatment for COVID-19 to receive FDA approval. The FDA first issued an EUA for Olumiant in combination with remdesivir to treat COVID-19 in hospitalized adults and pediatric patients on November 19, 2020. On July 28, 2021, the FDA revised the EUA to authorize Olumiant as a standalone treatment. Baricitinib is a Janus kinase (JAK) inhibitor that was previously approved for treatment of rheumatoid arthritis. The efficacy and safety of baricitinib were assessed in 2 Phase 3, randomized, double-blind, placebo-controlled clinical trials that compared baricitinib to placebo plus “background standard of care” in hospitalized patients requiring supplemental oxygen. In the larger of the two trials, which included 1525 patients, the estimated proportion of patients who died or progressed to non-invasive ventilation/high-flow oxygen or invasive mechanical ventilation was lower in patients treated with baricitinib (27.8%) compared to placebo (30.5%), but this effect was not statistically significant [odds ratio: 0.85 (95% CI 0.67, 1.08); p = 0.180]. The proportion of patients who died by Day 28 was 8.1% (62/764) for baricitinib compared to 13.3% (101/761) for placebo [estimated difference in Day 28 probability of mortality = -4.9% (95% CI: -8.0%, -1.9%); hazard ratio = 0.56 (95% CI: 0.41, 0.77)].
The Alaska DHSS website on COVID-19 therapeutics is regularly updated for providers and has everything you need to evaluate which therapeutic is right for your patient and the tools to prescribe these medications.
Evusheld (tixagevimab-cilgavimab) appears to reduce risk of severe COVID-19 or death by 50.5% among unvaccinated persons
In this phase 3 randomized, double-blind, placebo-controlled study conducted at 95 sites in the USA, Latin America, Europe, and Japan, researchers evaluate the safety and efficacy of tixagevimab-cilgavimab in preventing severe COVID-19 or death. This trial enrolled 910 participants from January-July 2021. Severe COVID-19 or death occurred in 18 (4%) of 407 participants in the tixagevimab–cilgavimab group versus 37 (9%) of 415 participants in the placebo group (relative risk reduction 50·5% [95% CI 14·6–71·3]; p=0·0096). The absolute risk reduction was 4·5% (95% CI 1·1–8·0; p<0·0001). Adverse events occurred in 132 (29%) of 452 participants in the tixagevimab–cilgavimab group and 163 (36%) of 451 participants in the placebo group and were mostly of mild or moderate severity. There were three COVID-19-reported deaths in the tixagevimab–cilgavimab group and six in the placebo group. This medication is administered as a single intramuscular injection.
Inaccurate pulse oximetry may overestimate arterial oxygen saturation levels in Asian, Black, and Hispanic patients compared to White patients and may contribute to unrecognized or delayed recognition of hypoxemia
In this retrospective analysis of medical records in a registry of five hospitals in the Johns Hopkins Health System, researchers included 1216 patients with concurrently measured SpO2 and SaO2 levels during their hospital encounter to evaluate whether there are systemic racial and ethnic biases in pulse oximetry among patients with COVID-19 and do these biases affect therapy. The median SaO2 for Asian and Black patients was consistently lower than the SpO2 value (ie, SpO2 overestimated the true oxygen saturation) for all SpO2 readings of 88% to 96%, while the median SaO2 was consistently higher than the SpO2 value (SpO2 underestimated the true oxygen saturation) for White patients with an SpO2 of 88% to 96%. Using the unadjusted linear mixed-effects model that was limited to SpO2 values from 88% to 96%, compared with White patients, SpO2 overestimated SaO2 by 2.1% for Asian patients, 1.4% for Black patients, and 0.8% for non-Black Hispanic patients. Occult hypoxemia (SaO2 <88% with concurrent SpO2 measurement of 92%-96%) was identified in 3.7% of samples from Asian patients, 3.7% of samples from Black patients, 2.8% of samples from non-Black Hispanic patients, and 1.7% of samples from White patients. When comparing pulse oximetry measurements with arterial oxygen saturation, approximately one-third of patients from each racial or ethnic minority group had at least 1 unidentified episode of hypoxia compared with fewer than one-fifth of White patients. In addition, we found a systematic failure to identify Black and Hispanic patients who were likely qualified to receive COVID-19 therapy and a statistically significant delay in recognizing the guideline-recommended threshold for initiation of therapy among Black patients compared with White patients.
Paxlovid associated with reduced COVID-19 hospitalization and death during Omicron surge in Israel in 2 different studies
In this observational, retrospective cohort study, authors assessed the real-world efficacy of Paxlovid (nirmatrelvir+ritonavir) for preventing COVID-19 hospitalization and death due to the Omicron variant. Data obtained from the electronic medical records of Clalit Health Services (CHS), a large healthcare organization covering approximately 52% of the entire Israeli population and almost two-thirds of the older adults, included 109,213 participants who were eligible for paxlovid therapy during the two-month study period. Among the 42,819 eligible patients aged 65 years and above, 2,504 were treated with paxlovid. Hospitalizations due to Covid-19 occurred in 14 out of the treated and 762 of the untreated patients: adjusted HR 0.33 (95% CI, 0.19 to 0.55). Death due to Covid-19 occurred in 2 treated and 151 untreated patients; adjusted HR: 0.19 (95% CI, 0.05 to 0.76). Among the 66,394 eligible patients 40 to 64 years of age, 1,435 were treated with paxlovid. Hospitalizations due to Covid-19 occurred in 9 treated and 334 untreated patients: adjusted HR 0.78 (95% CI, 0.40 to 1.53). Death due to Covid-19 occurred in 1 treated and 13 untreated patients; adjusted HR: 1.64 (95% CI, 0.40 to 12.95). The authors concluded that paxlovid therapy was associated with a 67% reduction in Covid-19 hospitalizations and an 81% reduction in Covid-19 mortality in patients 65 years and above. However, no significant benefit in avoidance of severe Covid-19 outcomes was shown in younger adults.
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
In another observational retrospective cohort study, authors used data from Israel’s largest healthcare provider to evaluate the real-world efficacy of Paxlovid in January-February 2022. Researchers identified all adults with first ever positive test for COVID between January-February 20222 who were at high risk for severe COVID-19 and had no contraindications for Paxlovid use. Patients were included irrespective of their COVID-19 vaccination status. Overall, 180,351 eligible were included, of them only 4,737 (2.6%) were treated with Paxlovid, and 135,482 (75.1%) had adequate COVID-19 vaccination status. Both Paxlovid and adequate COVID-19 vaccination status were associated with significant decrease in the rate of severe COVID-19 or mortality with adjusted HR 0.54 (95% CI, 0.39-0.75) and 0.20 (95% CI, 0.17-0.22), respectively. Paxlovid appears to be more effective in older patients, immunosuppressed patients, and patients with underlying neurological or cardiovascular disease (interaction p-value <0.05 for all).
Most COVID infections were not persistently asymptomatic and asymptomatic infections were less infectious than symptomatic infections
In this living systematic review and meta-analysis of 130 studies, researchers recently updated the review to address 3 questions: what proportion of people infected with SARS-CoV-2 never experience symptoms, what is the infectiousness of asymptomatic and presymptomatic infections, and what proportion of SARS-CoV-2 transmission is accounted for by people who are asympomatic or presymptomatic? The authors conclude that based on studies published up to July 2021, most SARS-CoV-2 infections were not persistently asymptomatic, and asymptomatic infections were less infectious than symptomatic infections.
Home COVID antigen test was 64% sensitive compared to RT-PCR; sensitivity peaked 4 days after illness onset; second test 1-2 days later showed improved sensitivity
In this prospective cohort study of 225 adults, participants with recent RT-PCR-confirmed SARS-CoV-2 infection were offered home antigen tests (Quidel QuickVue At-Home OTC COVID-19 test) and asked to perform 1 antigen test daily to evaluate antigen test sensitivity against RT-PCR and viral culture. The 225 enrolled cases contributed 3044 home antigen tests and 642 NP swabs, including 593 pairs of antigen tests and NP swabs that were performed on the same date. The daily positivity during the infectious period of cases peaked at 95% for RT-PCR tests (3 days after illness onset), 77% for antigen tests (4 days after illness onset), and 64% for viral cultures (2 days after illness onset). The daily positivity decreased more quickly for the antigen test and culture compared with RT-PCR. Six days after illness onset, when people with mild or asymptomatic SARS-CoV-2 infection may discontinue isolation according to current CDC guidance, RT-PCR positivity was 86%, antigen test positivity was 61%, and culture positivity was 36%. At 11 days after illness onset, when most individuals are no longer considered infectious, RT-PCR positivity remained high (86%), while antigen test positivity and culture positivity were low (16% and 9%, respectively). Overall sensitivity of home antigen tests for detecting cases was 50% (95% CI, 45%-55%), whereas specificity was 97% (95% CI, 95%-98%). Sensitivity was higher for symptomatic cases (53%; 95% CI, 48%-57%) compared with asymptomatic cases (20%; 95% CI, 10%-35%). The sensitivity of antigen tests was 64% (95% CI, 56%-70%) compared with RT-PCR tests collected on the same day. Home antigen test sensitivity peaked 4 days after illness onset. Sensitivity improved when a second antigen test was performed 1 to 2 days later, particularly early in the illness course. More than half of those who performed antigen tests on day 6 of illness had positive test results, but by day 11, fewer than one-fifth had positive test results.
COVID-19 booster vaccination associated with reduction in incident infections during Omicron wave
In this observational retrospective cohort study, researchers used a cohort of NBA players and staff to evaluate the incidence of SARS-CoV-2 infection from December 1, 2021 to January 15, 2022 in those who did versus those who did not receive a booster vaccine. Of 2613 players and staff, 67% were followed up the entire 45-day study period. From the start to the end of the study period, the percentage of individuals who were fully vaccinated and eligible for a booster dose decreased from 26% (n = 682) to 8% (n = 205) and the percentage of individuals who were fully boosted increased from 49% (n = 1282) to 85% (n = 2215). In the overall cohort, 88% were male with a median age of 33.7 years (IQR, 27.3-45.2 years). Individuals who were fully boosted experienced 608 confirmed SARS-CoV-2 infections and were significantly less likely to be infected than fully vaccinated individuals who were booster eligible and had not received a booster, who had experienced 127 confirmed infections (adjusted HR, 0.43 [95% CI, 0.35-0.53], P < .001). The secondary analyses evaluating symptomatic infection showed a similar association (adjusted HR, 0.39 [95% CI, 0.30-0.50]; P < .001). No hospitalizations or deaths occurred. Omicron was the dominant variant, representing 93% of 339 sequenced cases.
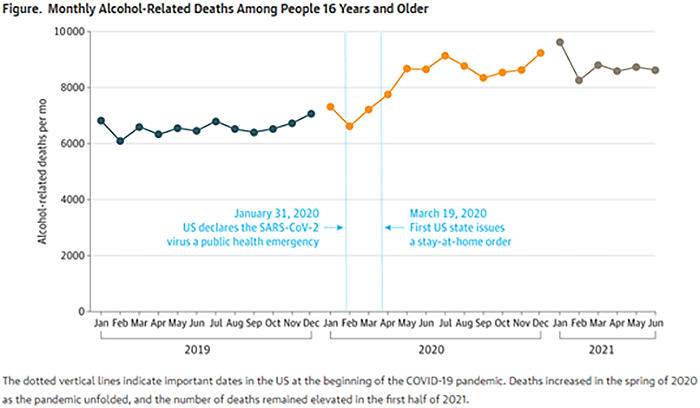
Number and rate of alcohol-related deaths increased 25% between 2019 and 2020
In this JAMA research letter, authors examined mortality data to assess whether alcohol-related deaths increased during the first year of the COVID-19 pandemic. The number of deaths involving alcohol increased between 2019 and 2020 (from 78 927 to 99 017 [relative change, 25.5%]), as did the age-adjusted rate (from 27.3 to 34.4 per 100 000 [relative change, 25.9%]). Comparatively, deaths from all causes had smaller relative increases in number (from 2 823 460 to 3 353 547 [18.8%]) and rate (from 938.3 to 1094.3 per 100 000 [16.6%]). Alcohol-related deaths accounted for 2.8% of all deaths in 2019 and 3.0% in 2020. Rates increased for all age groups, with the largest increases occurring for people aged 35 to 44 years (from 22.9 to 32.0 per 100 000 [39.7%]) and 25 to 34 years (from 11.8 to 16.1 per 100 000 [37.0%]). Increases in rates were similar for females and males.
Omicron variant associated with higher death rate for elderly
In an article for the New York Times, reporters highlight the rising death rate for people 65 and older during the Omicron wave – “Almost as many Americans 65 and older died in four months of the Omicron surge as did in six months of the Delta wave.”
1 million COVID-19 Deaths in the US
On May 9, the Washington National Cathedral rang its bell 1,000 times – once for each 1,000 American lives lost to COVID-19.
Alaska Epidemiology Bulletin – Critical Congenital Heart Disease, Prevalence and Detection
Published on May 9, this Alaska Epidemiology Bulletin characterizes the prevalence of critical congenital heart defects (CCHD), as well as the methods and timing of clinical detection, from 2007-2018. Alaska prevalence estimates for each CCHD were either lower or comparable to national estimates. The prevalence of CCHDs was equivalent across maternal age and race and no geographic clustering was detected. For all confirmed cases of CCHDs, 46.2% were detected prenatally, 24.9% were detected soon after birth during the clinical assessment, 3.6% were detected via pulse oximeter screening at 24-hours post birth, and 23.5% were not detected until after 24-hours after birth (in some cases several months after discharge). Coarctation of the aorta (39%) and Tetralogy of Fallot (25%) accounted for the majority of late CCHD diagnoses.
MMWRs
Alaska Native/American Indian persons living in Alaska are at increased risk for COVID-19 illness, COVID-19–associated hospitalization, and COVID-19–related death compared with White persons living in Alaska
In this MMWR, authors performed a retrospective analysis of COVID-19 cases reported to the Alaska Department of Health and Social Services during March 12, 2020–December 31, 2021, to examine the extent of COVID-19–associated disparities among Alaska Native/American Indian (AN/AI) persons living in Alaska. The age-adjusted COVID-19 incidence among AN/AI persons was 26,583 per 100,000 standard population, approximately twice the rate among White persons living in Alaska (11,935). The age-adjusted COVID-19–associated hospitalization rate among AN/AI persons was 742 per 100,000, nearly three times the rate among White persons (273) (rate ratio [RR] = 2.72). The age-adjusted COVID-19–related mortality rate among AN/AI persons was 297 per 100,000, approximately three times that among White persons (104; RR = 2.86). Culturally competent public health efforts that are designed in collaboration with AN/AI persons and communities, including support for vaccination and other proven COVID-19 prevention or treatment strategies, are critical to reducing COVID-19–associated disparities among Alaska Native/American Indian persons in Alaska.
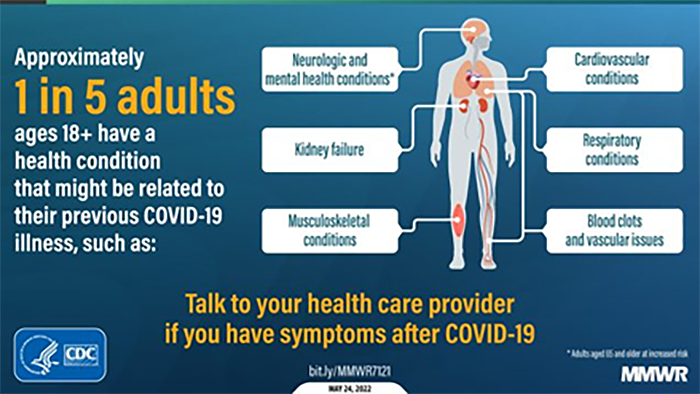
COVID survivors at significant risk of post-COVID conditions - twice the risk of pulmonary embolism or a respiratory condition and 20-25% incidence of one condition that may be attributable to prior COVID-19
In this MMWR, researchers performed a retrospective matched cohort design to analyze EHRs during March 2020–November 2021 to assess the incidence of 26 conditions often attributable to post-acute sequelae of COVID among patients who had received a previous COVID-19 diagnosis (case-patients) compared with the incidence among matched patients without evidence of COVID-19 in the EHR (control patients). Data were drawn from Cerner Real-World Data, a data set of approximately 63.4 million unique adult records from 110 data contributors in the 50 states
Case-patients (353,164) were adults aged ≥18 years who received either a diagnosis of COVID-19 or a positive SARS-CoV-2 test. Control patients (1,640,776) had a visit in the same month as the matched case-patient and did not receive a COVID-19 diagnosis or a positive SARS-CoV-2 test result during the observation period. Controls were matched 5:1 with case-patients. Among all patients aged ≥18 years, 38% of case-patients experienced an incident condition compared with 16% of controls; conditions affected multiple systems, and included cardiovascular, pulmonary, hematologic, renal, endocrine, gastrointestinal, musculoskeletal, neurologic, and psychiatric signs and symptoms. By age group, the highest risk ratios (RRs) were for acute pulmonary embolism (RR = 2.1 and 2.2 among persons aged 18–64 and ≥65 years, respectively) and respiratory signs and symptoms (RR = 2.1 in both age groups). Among those aged 18–64 years, 35.4% of case-patients experienced an incident condition compared with 14.6% of controls. Among those aged ≥65 years, 45.4% of case-patients experienced an incident condition compared with 18.5% of controls. These findings translate to one in five COVID-19 survivors aged 18–64 years, and one in four survivors aged ≥65 years experiencing an incident condition that might be attributable to previous COVID-19.
In nursing home setting, COVID-19 mRNA booster vaccine was 46.9% effective at preventing COVID-19 during Omicron predominance
Using data from the CDC’s National Healthcare Safety Network (NHSN) during February 14–March 27, 2022, when the Omicron variant was predominant, authors estimated the relative vaccine efficacy (VE) against infection for any COVID-19 additional primary or booster dose compared with primary series vaccination for persons residing in a skilled nursing facility (SNF). After adjusting for calendar week and variability across skilled nursing facilities, relative VE of a COVID-19 additional primary or booster dose was 46.9% (95% CI = 44.8%–48.9%). Infection rates among residents who received an additional or booster dose were compared with those who received primary series vaccination only to estimate relative additional or booster dose VE. After applying exclusion criteria and pairing SNF-level weekly case with corresponding resident data, the analysis included 85,494 reports from 14,758 SNFs. 22% of respondents had received primary series vaccination only, and 65% of whom had received an additional or booster dose. Among residents who had received primary series vaccination or an additional or booster dose, >90% had received mRNA COVID-19 vaccines. Crude weekly confirmed SARS-CoV-2 infection rates declined across all vaccination groups during the study period; however, rates of infection among residents with an additional or booster dose were consistently lower than those among residents with primary series vaccination only or among unvaccinated residents. Overall, 7,510 cases were confirmed among 1,509,674 resident-weeks with primary series vaccination only and 11,334 cases were confirmed among 4,416,401 resident-weeks with an additional or booster dose. The adjusted relative VE against infection for an additional or booster dose versus primary series vaccination only was 46.9%.
RECURRENT TOPICS
Providing COVID-19 vaccinations
All Alaskans and people who work or live in Alaska who are aged 5 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Free self-paced online course available to promote COVID-19 vaccine confidence in Alaskan Communities
Two online courses are available for free through the UAA Alaska Center for Rural Health & Health Workforce in partnership with the State of Alaska Department of Health and Social Services Division of Public Health. These courses are designed to provide participants the knowledge and skills to promote COVID-19 vaccine confidence among clients, family, friends, patients and/or community members in Alaskan communities. For those who complete the online course, there is an option to attend the live practical session to apply what they learned. These will occur monthly until the end of June and the live sessions are also free.
The Provider course is designed for licensed, or license eligible healthcare providers (1 contact hour, Interprofessional Continuing Education credit [ANMC]).
The Community course is aimed at entry level healthcare professionals and the interested public (3 hours)
Oral COVID-19 Antivirals
The FDA has authorized two oral antivirals – Paxlovid and Molnupiravir - for the treatment of mild-to-moderate COVID-19 in adults 18 years and older who are at high risk for progression to severe COVID-19. Paxlovid is also authorized for children age 12-17 years.
Monoclonal Antibodies
Currently, only Eli Lilly’s bebtelovimab monoclonal antibody shows high activity against the BA.2 Omicron subvariant. It is approved to treat mild-moderate COVID-19 in individuals who are at high risk for progression to severe COVID-19.
Evusheld (tixagevimab/cilgavimab) is recommended for SARS-CoV-2 pre-exposure prophylaxis (PrEP) for adults and adolescents (aged ≥12 years) who do not have SARS-CoV-2 infection, who have not been recently exposed to an individual with SARS-CoV-2 infection, AND who are moderately to severely immunocompromised or are not able to be fully vaccinated with any available COVID-19 vaccines due to a history of severe adverse reactions to a COVD-19 vaccine.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the NIH COVID-19 Treatment Guidelines
Evusheld led to lower incidence of COVID-19 infection, hospitalization, and death in VA patients during Omicron surge
In a retrospective analysis of data from Veterans Affairs, researchers attempted to determine the effectiveness of tixagevimab/cilgavimab for prevention of SARS-CoV-2 infection and severe disease among immunocompromised patients. Authors compared a cohort of 1,848 patients treated with at least one dose of intramuscular tixagevimab/cilgavimab to matched controls selected from 251,756 patients who were on immunocompromised or otherwise at high risk for COVID-19. Patients were followed through April 30, 2022, or until death, whichever occurred earlier. Most (69%) tixagevimab/cilgavimab recipients were ≥65 years old, 92% were identified as immunocompromised in electronic data, and 73% had ≥3 mRNA vaccine doses or two doses of Johnson & Johnson. Compared to propensity-matched controls, tixagevimab/cilgavimab-treated patients had a lower incidence of the composite COVID-19 outcome (17/1733 [1.0%] vs 206/6354 [3.2%]; HR 0.31; 95%CI, 0.18-0.53), and individually SARS-CoV-2 infection (HR 0.34; 95%CI, 0.13-0.87), COVID-19 hospitalization (HR 0.13; 95%CI, 0.02-0.99), and all-cause mortality (HR 0.36; 95%CI, 0.18-0.73).
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
Pregnancy
The CDC strongly recommends COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology. In addition, JAMA has published a one-page patient information sheet on COVID-19 and pregnancy.
Post-acute Sequelae of COVID-19 (PASC)
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions. This page was most recently updated on May 5.
Bartlett Regional Hospital launches new telehealth rehabilitation program for patients with long-term effects of COVID-19 or COPD
Bartlett Regional Hospital in Juneau has expanded its pulmonary rehabilitation program to include a fully remote option for patients who suffer from long-term effects of COVID-19 or chronic obstructive pulmonary disease (COPD). Telehealth pulmonary rehabilitation is a live and interactive online class, which allows patients to exercise and receive education and support from the comfort of their own home, under the guidance of a registered respiratory therapist and exercise physiologist.
Patients with COPD and post COVID-19 symptoms that include difficulty breathing for over four weeks may be eligible to enroll. Provider referral is required. Individuals interested in receiving more information are encouraged to talk to their primary healthcare provider or contact Bartlett’s Pulmonary Rehabilitation Team at CPrehab@bartletthospital.org or (907) 796-8495.
23% of COVID-19 patients had at least one post-COVID condition, more post-COVID conditions associated with females than males, and increased odds of death 30 days or more for those hospitalized for COVID
In this white paper from FAIR Health, a database of more than 34 billion healthcare claims, authors studied
a total of 1,959,982 COVID-19 patients for the prevalence of post-COVID conditions 30 days or more after their initial diagnosis with COVID-19. Of patients who had COVID-19, 23.2 percent had at least one post-COVID condition. Post-COVID conditions were found to a greater extent in patients who had more severe cases of COVID-19, but also in a substantial share of patients whose cases lacked symptoms. Of patients who were hospitalized with COVID-19, the percentage that had a post-COVID condition was 50%; of patients who were symptomatic but not hospitalized, 27.5%; and of patients who were asymptomatic, 19%.The five most common post-COVID conditions across all ages, in order from most to least common, were pain, breathing difficulties, hyperlipidemia, malaise and fatigue, and hypertension. Most of the post-COVID conditions that were evaluated were associated more with females than
males. The odds of death 30 days or more after initial diagnosis with COVID-19 were 46 times higher for patients who were hospitalized with COVID-19 and discharged than patients who had not been hospitalized (odds ratio [OR]=46.020, 95 percent confidence interval [CI], 34.778-60.897,
P<0.001). Of COVID-19 patients who were hospitalized and discharged, 0.5 percent died 30 days
or more after their initial diagnosis. Among COVID-19 patients with preexisting conditions, intellectual disabilities were associated with the highest odds of death 30 days or more after initial COVID-19 diagnosis (OR=3.082, 95
percent CI, 1.183-8.029, P=0.0212).
*This article has not gone through peer review and is published as a white paper. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 in Alaska.
Aside from COVID-19
Project Firstline
If you or your organization are interested in learning more about infection control in health care, the CDC has a robust training collaborative and resource library under Project Firstline. If you’re interested in learning more about Project Firstline or potentially arranging a training session, please contact Kelley O’Leary at kelley.oleary@alaska.gov
Provider Relief Fund – Request to report late
The Provider Relief Fund (PRF) Request to Report Late Due to Extenuating Circumstances process is intended for providers who were required to report in an applicable reporting period, but extenuating circumstances prevented them from submitting a report by the required deadline. For each PRF Reporting Period, a provider may request an opportunity to complete their report after the reporting period deadline based on attestation that one of the following allowable extenuating circumstances applies at the time of the deadline: severe illness or death, impacted by natural disaster, lack of receipt of reporting communications, failure to click “submit,” internal miscommunication or error, or incomplete targeted distribution payments.
CDC Health Advisory: Recommendations for Adenovirus Testing and Reporting of Children
with Acute Hepatitis of Unknown Etiology
On April 21, the CDC released a Health Advisory for US clinicians who may encounter pediatric patients with hepatitis of unknown etiology to consider adenovirus testing and to elicit reporting of such cases to state public health
authorities and to CDC. In November 2021, clinicians at a large children’s hospital in Alabama notified the CDC of five pediatric patients with significant liver injury, including three with acute liver failure, who also tested positive for adenovirus. All children were previously healthy. None had COVID-19. Two patients required liver transplant; no patients died. A possible association between pediatric hepatitis and adenovirus infection is currently under investigation.
Public Naloxone Training
DHSS OSMAP Project HOPE are conducting public naloxone trainings as a community outreach and to increase awareness and access. Email projecthope@alaska.gov.
Harm reduction strategies and resources
The Alaska Native Tribal Health Consortium (ANTHC) HIV/STD Prevention and Substance Misuse Prevention programs host free virtual gatherings to discuss harm reduction strategies and resources in Alaska. Guest speakers are Alaska-based experts in the field of harm reduction. Recordings of harm reduction trainings can be found here.
Several useful materials specific to Alaska opioid safety are at the following webpage. Check it out and print out information to hang up in your community.
Events/Conferences/Presentations
CDC COCA Call – What Clinicians Need to Know About Available Therapeutic Options for COVID-19
On June 16, from 2-3pm EST, subject matter experts will present an overview of COVID-19 therapeutic options, including indications, efficacy, and distribution.
When:
Thursday, June 16, 2022,
2:00 PM – 3:00 PM ET
Webinar Link:
https://www.zoomgov.com/j/1603960029
Passcode: 308026
Dial In:
US: +1 669 254 5252
or +1 646 828 7666
or +1 551 285 1373
or +1 669 216 1590
International numbers
One-tap mobile:
US: +16692545252,,1603960029#,,,,*308026# or +16468287666,,1603960029#,,,,*308026#
Webinar ID: 160 396 0029
CDC COCA Call – Clinical Recommendations for Adenovirus Testing and Reporting of Children with Acute Hepatitis of Unknown Etiology – May 19, 2022
The CDC is investigating a cluster of children identified with hepatitis and adenovirus infection. While there have been case reports of hepatitis in immunocompromised children with adenovirus type 41 infection in the past, adenovirus type 41 is not known to be a cause of hepatitis in otherwise healthy children. More common causes for hepatitis have been ruled out. During this COCA Call, presenters discussed the unknown etiology of patients under investigation, progress of the investigation, and how clinicians can continue to support these efforts through testing and reporting.
CDC COCA Call - Evaluating and Supporting Patients Presenting with Cognitive Symptoms Following COVID – May 5, 2022
Presenters discussed post-COVID conditions (PCC), an umbrella term for the wide range of health consequences that are present four or more weeks after infection with SARS-CoV-2, which includes long COVID.
Drug Addiction Treatment Act (DATA) Waivers ECHO
UAA Center for Human Development and the State of Alaska Division of Behavioral Health are pleased to offer a new Project ECHO for medical providers who are currently DATA waivered and/or medical providers who are interested in obtaining a DATA waiver.
July 13 at 12:00pm Tapering or stopping buprenorphine treatment
August 10 at 12:00pm Prenatal/OB MAT
Sept 14 at 12:00pm Understanding and reducing buprenorphine diversion
Registration link for DATA Waivers ECHO:
https://echo.zoom.us/meeting/register/tJYqce-gqDovGdDitNu5EPxMU1UOPrBth7Wv
Hosted and facilitated by UAA’S Center for Human Development Alaska ECHO Project in partnership with the State of Alaska Division of Behavioral Health. For questions, please contact echo@alaskachd.org
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. There are no webinars throughout the remainder of June or in the month of July since many individuals will be participating in subsistence activities during these months. The series will resume in August.
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
The most up-to-date, evidence based COVID-19 treatment guidelines can be found at:
NIH COVID-19 Treatment Guidelines
IDSA Guidelines on the Treatment and Management of Patient with COVID-19
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
|
