COVID-19 Alaska Clinical Update – April 8
Friday, April 8
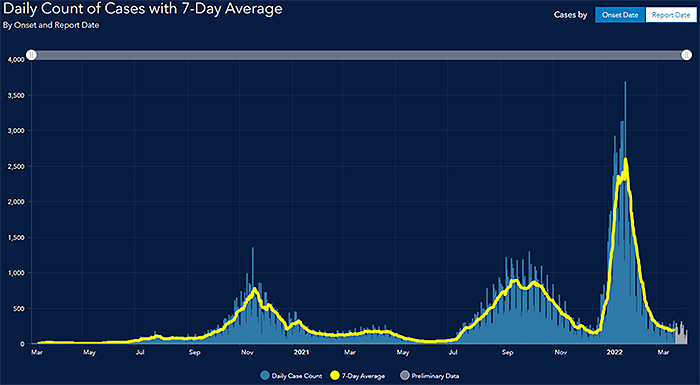
Graph taken from State of Alaska’s COVID-19 Cases Dashboard
Changes to Alaska community alert levels and COVID-19 data reporting
DHSS has reviewed how CDC’s new COVID-19 community levels may apply to Alaska. The community levels are useful because they consider hospitalizations and are not solely based on case data. However, we encourage the public and community leaders to continue to be aware of case rates in concert with the community levels. Community levels alone may not fully capture risk associated with localized high levels of transmission, especially in rural areas. Beginning this week, the Alert Levels on the dashboard have been replaced by Case Rate Levels. Moving forward, DHSS will be updating data on the Alaska COVID-19 Information Hub once a week.
FDA limits use of monoclonal antibody Sotrovimab
The FDA has revised the emergency use authorization for sotrovimab to clarify that sotrovimab is not authorized for treatment of mild-to-moderate COVID-19 in geographic regions where COVID-19 infection is likely to have been caused by the Omicron subvariant BA.2, which is not susceptible to treatment with sotrovimab. As of April 5th, 2022, sotrovimab is no longer authorized for use in the United States. For the week ended 3/13/22, BA.2 accounted for 64.56% of cases sequenced in Alaska. The most up-to-date information regarding COVID-19 variants in Alaska is available on the COVID-19 Cases Dashboard under the COVID-19 Variants Tab.
FDA authorizes second booster of mRNA vaccine for adults 50 years and older and immunocompromised
On March 29, the FDA authorized a second booster dose of either the Pfizer-BioNTech or the Moderna COVID-19 vaccines for older people and certain immunocompromised individuals. The second booster dose may be administered to adults 50 years and older at least 4 months after receipt of a first booster. Both the Moderna and Pfizer-BioNTech vaccines may be administered to individuals with immunocompromise, such as those who have undergone solid organ transplantation, or who are living with conditions that are considered to have an equivalent level of immunocompromise. The Moderna vaccine is authorized for immunocompromised individuals 18 years and older, while the Pfizer-BioNTech vaccine is authorized for immunocompromised individuals 12 years and older.
Monoclonal antibodies most effective when used prophylactically or early in illness
In this pre-print study that has not yet been peer-reviewed, researchers performed a meta-analysis of 37 randomized controlled trials to investigate how the timing and dose of passive antibodies predicts protection from SARS-CoV-2 infection. Results show that both prophylactic and early therapeutic administration (to symptomatic ambulant subjects) have significant efficacy in preventing infection or progression to hospitalization respectively. However, authors found that effectiveness of passive antibody therapy in preventing clinical progression is significantly reduced with administration at later clinical stages (p<0.0001). The timing of antibody administration is a major factor in determining the success of treatment. For example, for the same antibody doses they saw 92.4% protection from infection when given as prophylaxis, but only 73.5% protection from progression to hospitalization when given to ambulatory outpatient COVID-19 patients, and negligible protection when given to hospitalized subjects. In addition, authors says their results predict that the dose of monoclonal antibody required to prevent progression to severe SARS-CoV-2 infection is likely significantly lower than that administered in most current treatment schedules and suggest that if the efficacy of low-dose antibodies can be demonstrated, this would significantly reduce costs and may facilitate alternative modes of administration.
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
Following COVID-19 infection, 40% increased risk of diabetes
Using the national databases of the US Department of Veterans Affairs, researchers examined the post-acute risk and burden of incident diabetes in people who survived the first 30 days of SARS-CoV-2 infection. The study population consisted of a cohort of 181,280 participants who had a positive COVID-19 test between March 2020 and Sept 2021, and survived the first 30 days of COVID-19; a contemporary control (n=4,118,441) that enrolled participants between March 2020, and Sept 2021; and a historical control (n=4,286,911) that enrolled participants between March 2018, and Sept 2019. Both control groups had no evidence of SARS-CoV-2 infection. Participants in all three comparison groups were free of diabetes before cohort entry and were followed up for a median of 352 days. In the post-acute phase of the disease, compared with the contemporary control group, people with COVID-19 exhibited an increased risk (HR 1.40, 95% CI 1.36–1.44) and excess burden (13.46, 95% CI 12.11–14.84, per 1000 people at 12 months) of incident diabetes; and an increased risk (1.85, 1.78–1.92) and excess burden (12.35, 11.36–13.38) of incident antihyperglycemic use. Additionally, analyses to estimate the risk of a composite endpoint of incident diabetes or antihyperglycemic use yielded a HR of 1.46 (95% CI 1.43–1.50) and an excess burden of 18.03 (95% CI 16.59–19.51) per 1000 people at 12 months. Risks and burdens of post-acute outcomes increased in a graded fashion according to the severity of the acute phase of COVID-19 (whether patients were non-hospitalized, hospitalized, or admitted to intensive care). All the results were consistent in analyses using the historical control as the reference category. Authors conclude that altogether, these results indicate that beyond the acute phase of COVID-19, survivors are at an increased risk of developing incident diabetes and antihyperglycemic use; therefore diabetes should be considered as a component of the multifaceted long COVID.
Israeli study shows significant reduction in COVID-19 mortality following receipt of second booster for adults 60 years and older
In this pre-print study that has not yet been peer-reviewed, authors performed a retrospective cohort study to evaluate mortality due to COVID-19 in Israeli adults aged 60 to 100 who received a second COVID mRNA booster vaccine compared to adults who only received a single booster. Following a rise in breakthrough infections caused by the omicron variant in individuals who had already received three vaccine doses, the Israeli Ministry of Health initiated a fourth vaccine dose campaign on January 2, 2022, available to all adults 60 years and older, high-risk populations, and healthcare workers who received a first booster dose at least four months earlier. In this study, which included all members of the Clalit Health Services who were eligible for a second booster, a total of 563,465 participants met the eligibility criteria. Of those, 328,597 (58%) received a second-booster dose during the 40-day study period. Death due to Covid-19 occurred in 92 second-booster recipients and in 232 participants who received one booster dose (adjusted hazard ratio 0.22; 95% confidence interval 0.17 to 0.28).
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
Treatment with ivermectin did not lead to lower incidence of hospitalization among COVID-19 patients
In this double-blind, randomized, placebo-controlled, adaptive platform trial involving symptomatic SARS-CoV-2–positive adults recruited from 12 public health clinics in Brazil, researchers evaluated the efficacy of ivermectin in preventing hospitalization or extended observation in an emergency setting among outpatients with acutely symptomatic COVID-19. Patients who had had symptoms of COVID-19 for up to 7 days and had at least one risk factor for disease progression were randomly assigned to receive ivermectin (400 μg/kg) once daily for 3 days or placebo. The primary composite outcome was hospitalization due to COVID-19 within 28 days after randomization or an emergency department visit due to clinical worsening of Covid-19 within 28 days after randomization. A total of 3515 patients were randomly assigned to receive ivermectin (679 patients), placebo (679), or another intervention (2157). Overall, 100 patients (14.7%) in the ivermectin group had a primary-outcome event, as compared with 111 (16.3%) in the placebo group (relative risk, 0.90; 95% Bayesian credible interval, 0.70 to 1.16). Of the 211 primary-outcome events, 171 (81.0%) were hospital admissions. The authors conclude that treatment with ivermectin did not result in a lower incidence of medical admission to a hospital due to progression of Covid-19 or of prolonged emergency department observation among outpatients with an early diagnosis of Covid-19.
Repeat rapid antigen test increased estimated accuracy from 38% to 92% for true-positive results
In this retrospective comparative effectiveness trial, researchers used data from an international service company based in New York City to compare the accuracy of single and repeat rapid antigen tests compared to RT-qPCR testing. A total of 179,127 participants underwent testing where asymptomatic workers were administered a rapid antigen test from November 2020 to October 2021. Those with a positive antigen test result were offered a second antigen test of a nasal swab specimen within an hour of the first test result. All nasal swab specimens were also sent to a CLIA–certified laboratory for confirmatory RT-qPCR testing using the Cepheid GeneXpert RT-qPCR assay. Estimated accuracy was calculated as the percentage of second antigen tests with a positive result for which the RT-qPCR test result was also positive. A total of 179 127 rapid SARS-CoV-2 antigen tests were performed, with a 0.35% positivity rate (623 positive antigen test results) between November 2020 and October 2021 (Table). Of 623 total positive test results, 238 (38%) were confirmed to be true positive and 385 (62%) false positive by RT-qPCR. Of the 623 tests with positive results, 569 (91%) were followed by a second rapid antigen test. When the result of the first antigen test was positive and the result of the second antigen test was negative (n = 345), RT-qPCR results were negative for 328 (95%). The overall estimated accuracy of a second antigen test was 94%. When a repeated rapid antigen test was offered to participants of an employee screening program, the estimated accuracy increased from 38% to 92% for true-positive results as determined by RT-qPCR for SARS-CoV-2.
Alaska Influenza Snapshot – March 20–March 26, 2022
The State of Alaska DHSS Section of Epidemiology publishes a weekly snapshot of influenza surveillance and activity during the flu season. The report from Week 12: March 20, 2022 – March 26, 2022 was recently published.
MMWRs
Hospitalization rates for children 4 years and younger were 5x higher during peak of Omicron compared with Delta
In this MMWR, authors used COVID-NET data to describe COVID-19–associated hospitalizations among U.S. infants and children aged 0–4 years since March 2020. During the period of Omicron predominance (December 19, 2021–February 19, 2022), weekly COVID-19–associated hospitalization rates per 100,000 infants and children aged 0–4 years peaked at 14.5 (week ending January 8, 2022); this Omicron-predominant period peak was approximately five times that during the period of SARS-CoV-2 B.1.617.2 (Delta) predominance (June 27–December 18, 2021, which peaked the week ending September 11, 2021). During Omicron predominance, 63% of hospitalized infants and children had no underlying medical conditions; infants aged <6 months accounted for 44% of hospitalizations, although no differences were observed in indicators of severity by age. During March 1, 2020–February 19, 2022, weekly hospitalization rates (hospitalized patients per 100,000 infants and children aged 0–4 years) peaked during Omicron predominance at 14.5. This peak hospitalization rate during Omicron predominance was approximately five times the peak during Delta predominance (2.9) (RR = 5.0; 95% CI = 3.8–6.8). Hospitalization rates among infants aged <6 months were approximately six times as high during the peak week of Omicron predominance (68.1) as during Delta predominance (11.1) (RR = 6.1; 95% CI = 3.9–10.0); Omicron-predominant versus Delta-predominant hospitalization RRs were also elevated among infants and children aged 6–23 months (16.9 versus 3.3; RR = 5.1; 95% CI = 3.1–8.5) and 2–4 years (4.7 versus 1.4; RR = 3.5; 95% CI = 2.0–6.3) (Figure). Monthly ICU admission rates were approximately 3.5 times as high during the Omicron predominance peak in January 2022 (10.6) as during the Delta predominance peak in September 2021 (3.0). Hospitalization rates among infants and children aged 0–4 years decreased by the week ending February 19, 2022 (3.9). Coinciding with Omicron predominance, COVID-19–associated hospitalization rates among infants and children aged 0–4 years reached the current highest level of the pandemic during early January 2022.
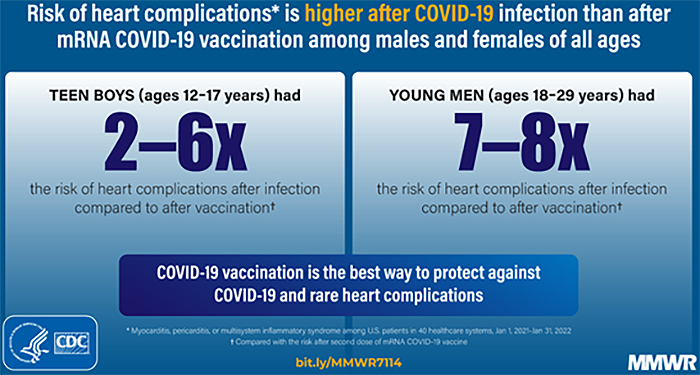
Risk of heart complications is higher following COVID-19 infection than after mRNA COVID-19 vaccination among males and females of all ages
In this MMWR, authors used data from 40 U.S. health care systems during January 1, 2021–January 31, 2022, to calculate incidences of cardiac outcomes (myocarditis; myocarditis or pericarditis; and myocarditis, pericarditis, or MIS) among persons aged ≥5 years who had SARS-CoV-2 infection, stratified by sex (male or female) and age group (5–11, 12–17, 18–29, and ≥30 years). Risk ratios (RR) were calculated to compare risk for cardiac outcomes after SARS-CoV-2 infection to that after mRNA COVID-19 vaccination. The incidence of cardiac outcomes after mRNA COVID-19 vaccination was highest for males aged 12–17 years after the second vaccine dose; however, within this demographic group, the risk for cardiac outcomes was 1.8–5.6 times as high after SARS-CoV-2 infection than after the second vaccine dose. The risk for cardiac outcomes was likewise significantly higher after SARS-CoV-2 infection than after first, second, or unspecified dose of mRNA COVID-19 vaccination for all other groups by sex and age (RR 2.2–115.2). The study population consisted of 15,215,178 persons aged ≥5 years, including 814,524 in the infection cohort; 2,548,334 in the first dose cohort; 2,483,597 in the second dose cohort; 1,681,169 in the unspecified dose cohort; and 6,713,100 in the any dose cohort. Among the four COVID-19 vaccination cohorts, 77%–79% of persons were aged ≥30 years; within the SARS-CoV-2 infection cohort, 63% were aged ≥30 years.
Use of at-home COVID-19 tests has rapidly increased but is lower among persons self-identified as Black, age 75 years or older, had lower incomes, or lower levels of education
As at-home COVID-19 tests become more widely available and used, laboratory-based reporting systems might increasingly underreport the actual incidence of infection. Data from a cross-sectional, nonprobability–based online survey (August 23, 2021–March 12, 2022) of U.S. adults aged ≥18 years were used to estimate self-reported at-home test use over time, and by demographic characteristics, geography, symptoms/syndromes, and reasons for testing. From the Delta-predominant period (August 23–December 11, 2021) to the Omicron-predominant period (December 19, 2021–March 12, 2022), at-home test use among respondents with self-reported COVID-19–like illness more than tripled from 5.7% to 20.1%. At-home test use differed by race (e.g., self-identified as White [5.9%] versus self-identified as Black [2.8%]), age (adults aged 30–39 years [6.4%] versus adults aged ≥75 years [3.6%]), household income (>$150,000 [9.5%] versus $50,000–$74,999 [4.7%]), education (postgraduate degree [8.4%] versus high school or less [3.5%]), and geography (New England division [9.6%] versus West South Central division [3.7%]).Since knowing if one has COVID-19 can allow for earlier treatment and protection for others, providing reliable and low-cost or free at-home test kits to underserved populations with otherwise limited access to COVID-19 testing could assist with continued prevention efforts. Among the surveyed population, the most common reported reasons for at-home test use were for risk assessments, such as COVID-19 exposure concerns (39.4%) and experiencing self-assessed COVID-19 symptoms (28.9%). Observed differences might reflect the price point, marketing, education, or disparities in availability and accessibility of at-home tests. Equitable access to COVID-19 testing is important to reduce disease spread.
RECURRENT TOPICS
Providing COVID-19 vaccinations
All Alaskans and people who work or live in Alaska who are aged 5 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Free self-paced online course available to promote COVID-19 vaccine confidence in Alaskan Communities
Two online courses are available for free through the UAA Alaska Center for Rural Health & Health Workforce in partnership with the State of Alaska Department of Health and Social Services Division of Public Health. These courses are designed to provide participants the knowledge and skills to promote COVID-19 vaccine confidence among clients, family, friends, patients and/or community members in Alaskan communities. For those who complete the online course, there is an option to attend the live practical session to apply what they learned. These will occur monthly until the end of June and the live sessions are also free.
The Provider course is designed for licensed, or license eligible healthcare providers (1 contact hour, Interprofessional Continuing Education credit [ANMC]).
The Community course is aimed at entry level healthcare professionals and the interested public (approximately 3 hours)
Oral COVID-19 Antivirals
The FDA has authorized two oral antivirals – Paxlovid and Molnupiravir - for the treatment of mild-to-moderate COVID-19 in adults 18 years and older who are at high risk for progression to severe COVID-19. Paxlovid is also authorized for children age 12-17 years.
The Alaska DHSS website on COVID-19 therapeutics has been updated for providers and has everything you need to evaluate which therapeutic is right for your patient and the tools to prescribe these medications.
Monoclonal Antibodies
Currently, only Eli Lilly’s bebtelovimab monoclonal antibody shows high activity against the BA.2 Omicron subvariant. It is approved to treat mild-moderate COVID-19 in individuals who are at high risk for progression to severe COVID-19.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the NIH COVID-19 Treatment Guidelines
Pregnancy
The CDC strongly recommends COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology. In addition, JAMA has published a one-page patient information sheet on COVID-19 and pregnancy.
Post-acute Sequelae of COVID-19 (PASC)
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 in Alaska.
Aside from COVID-19
Public Naloxone Training
DHSS OSMAP Project HOPE are conducting public naloxone trainings as a community outreach and to increase awareness and access. Email projecthope@alaska.gov.
Harm reduction strategies and resources
The Alaska Native Tribal Health Consortium (ANTHC) HIV/STD Prevention and Substance Misuse Prevention programs host free virtual gatherings to discuss harm reduction strategies and resources in Alaska. Guest speakers are Alaska-based experts in the field of harm reduction. Recordings of harm reduction trainings can be found here.
Several useful materials specific to Alaska opioid safety are at the following webpage. Check it out and print out information to hang up in your community.
CPT1A Arctic Variant Refresher
The CPT1A Arctic Variant is a genetic mutation that is commonly in many Alaska Native people. Among the Yu’pik and Inupiaq Alaska Native people it is the most common form of CPT1A. During an illness where children have reduced fluid and caloric intake, children with CPT1A Arctic Variant are at increased risk of hypoglycemia, seizures, and death. ANTHC has published a brief video explaining this condition for physicians, other health care providers, and anyone else interested. In addition, Dr. Matthew Hirschfeld, Medical Director of Maternal Child Health Services at Alaska Native Medical Center, has published slides from a recent presentation on CPT1A Arctic Variant and COVID-19 in Kids.
Caring for women Veterans in the community
Women Veterans are the fastest growing Veteran population in the VA healthcare system. They have unique health care needs that may require different assessments, care and resources compared to non-Veterans. For example, issues such as military sexual trauma, musculoskeletal pain, and post-deployment readjustment can impact women Veterans differently. To get the highest-quality care, women Veterans must have access to clinicians who are trained in women Veteran’s health. Community providers might not be aware of the special areas of concern that need to be addressed. To this end, the VA’s Office of Women’s Health has created a one-hour web-based training module Caring for Women Veterans which trains community care clinicians to provide Veteran and gender-specific care. Community Care Providers can take this training (CME available) and learn ways to talk about patients’ military history and address physical, mental, and reproductive health challenges unique to women Veterans.
Upcoming Events/Conferences/Presentations
Drug Addiction Treatment Act (DATA) Waivers ECHO
UAA Center for Human Development and the State of Alaska Division of Behavioral Health are pleased to offer a new Project ECHO for medical providers who are currently DATA waivered and/or medical providers who are interested in obtaining a DATA waiver.
April 13 at 12:00pm All things UDS/oral fluid tests for monitoring
May 11 at 12:00pm Behavioral Health - Psychosocial adjuncts to MAT
June 8 at 12:00pm Polysubstance use
July 13 at 12:00pm Tapering or stopping buprenorphine treatment
August 10 at 12:00pm Prenatal/OB MAT
Sept 14 at 12:00pm Understanding and reducing buprenorphine diversion
Registration link for DATA Waivers ECHO:
https://echo.zoom.us/meeting/register/tJYqce-gqDovGdDitNu5EPxMU1UOPrBth7Wv
Hosted and facilitated by UAA’S Center for Human Development Alaska ECHO Project in partnership with the State of Alaska Division of Behavioral Health. For questions, please contact echo@alaskachd.org
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule and the Zoom link.
April 8: Connie Jessen, MA. Alaska Indigenous Research Program Director. Alaska Stigma Index Project.
April 15: Eric Lim, MD. ANMC Orthopedics. Topic TBD
April 22: Leslie Kerzner, MD. Massachusetts General Hospital/Harvard Medical School. Neonatal Abstinence Syndrome for the Primary Care Provider.
April 29: Andrew Cornelius, MD. ANMC Orthopedics. Topic TBD.
May 6: Jessie Downes, MSN, DNP, RN. Alaska DHSS. Alaska Hypertension Program
Webinar Link: https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One-tap mobile: +16699006833,,98667611681#
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
The most up-to-date, evidence based COVID-19 treatment guidelines can be found at:
NIH COVID-19 Treatment Guidelines
IDSA Guidelines on the Treatment and Management of Patient with COVID-19
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
|
