COVID-19 Alaska Clinical Update
Wednesday, October 20, 2021
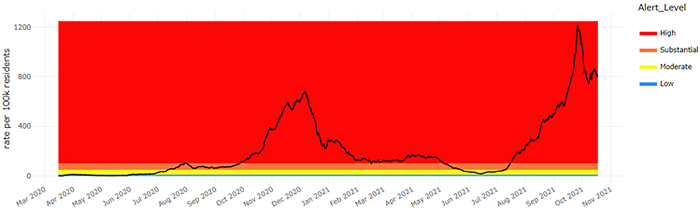
7-Day COVID-19 Case Rate – Statewide
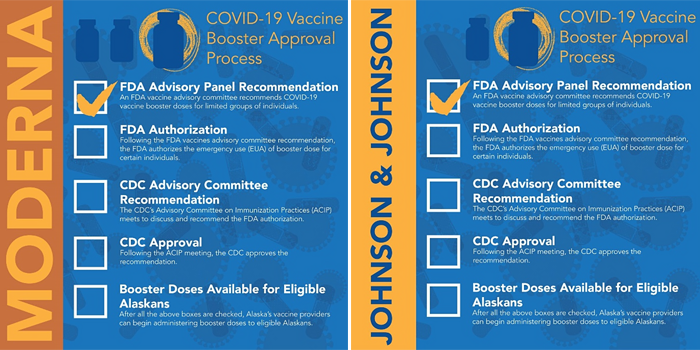
FDA’s VRBPAC recommends boosters for both Moderna and Johnson & Johnson
On October 14, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) unanimously voted to recommend a booster of Moderna’s COVID mRNA vaccine for the same high-risk populations that the Pfizer-BioNTech vaccine was recently authorized for. The booster vaccine is recommended for individuals aged 65 years and older, individuals aged 18 to 64 years old at high risk of severe COVID-19 or at high risk of frequent SARS-CoV-2 exposure due to institutional or occupational background. Unlike the Pfizer-BioNTech booster which is the same dose as the original vaccine series, the Moderna booster is a 50mcg injection, which is half of the dose of the initial vaccine.
On October 15, the FDA’s VRBPAC unanimously voted to recommend a booster of the Johnson & Johnson COVID vaccine for all persons age 18 years and older who received a single dose. Unlike the recommendations for Pfizer-BioNTech and Moderna, the committee recommended a booster dose for anyone who received the Johnson & Johnson vaccine, not just high-risk populations. The booster is recommended beginning two months after receiving the initial dose.
Before these booster become available to the public, they need to be authorized by the FDA, evaluated by the CDC’s Advisory Committee on Immunization Practices, and then received CDC approval.
The FDA’s VRBPAC has a meeting scheduled on October 26 to discuss Pfizer-BioNTech’s application to amend the EUA for its vaccines to allow the use of its COVID-19 vaccine in children aged 5 through 11 years.
Children may play larger role in COVID-19 transmission than previously assumed
In a prospective cohort study from Belgium, 63 children and 118 adults at one school had weekly testing for SARS-CoV-2 infection for 15 weeks. During the study period, 45 individuals (24.9%) tested positive: 13 children and 32 adults. Children were more often asymptomatic compared with adults (6 of 13 [46.2%] vs 4 of 31 [12.9%]). The median duration of symptoms was shorter in children than in adults (0.00 days [IQR, 0.00-1.00 days] vs 15.00 days [IQR, 7.00-22.00 days]). A reconstruction of the outbreak revealed that most transmission events occurred between teachers and between children within the school. Of the observed household transmission events, most seemed to have originated from a child or teacher who acquired the infection at school.
Physical inactivity associated with higher risk for severe COVID-19 outcomes
In this retrospective observational study of patients from the Kaiser Permanent Southern California health network, authors reviewed 48,440 adult patients with a COVID-19 diagnosis from January to October 2020, with at least three records of patients’ self-reported physical activity from March 2018 to March 2020, and then linked their physical activity category to the risk of hospitalization, ICU admission and death after COVID-19 diagnosis. Three categories of physical activity were created for this study based on the US Physical Activity Guidelines: consistently meeting guidelines (moderate to strenuous exercise >150 min/week at all assessments during the study period), consistently inactive (moderate to strenuous exercise 0–10 min/week at all assessments) and some activity (moderate to strenuous activity 11–149 min/week or those with variability in their exercise measures). Controlling for demographics and other risk factors for severe COVID-19, being consistently inactive resulted in significantly higher odds for the three outcomes compared with being either consistently meeting physical activity guidelines or doing some activity. Being consistently inactive increased the odds of hospitalization 2.26-fold (95% CI 1.18 to 2.83) compared with consistently meeting PA guidelines. Those who were doing some activity had 1.89 times greater odds of hospitalization (95% CI 1.53 to 2.33) than those who were consistently meeting PA guidelines. In addition, patients who were consistently inactive had greater odds of being hospitalized (OR 1.20; 95% CI 1.10 to 1.32) than patients who were doing some activity. Other than age, pregnancy, and a history of organ transplant, being consistently inactive conferred the highest odds for hospitalization with COVID-19. Patients who were consistently inactive had 1.73 times greater odds (95% CI 1.18 to 2.55) of ICU admission than patients who were consistently meeting physical activity guidelines. The odds of death were 2.49 times greater (95% CI 1.33 to 4.67) for patients who were consistently inactive compared with patients who were consistently meeting physical activity guidelines.
Compared to placebo, outpatient anticoagulation therapy did not reduce major cardiopulmonary adverse outcomes in people with symptomatic but stable SARS-CoV-2 infection
In this randomized, double-blind, placebo-controlled trial, 657 symptomatic outpatients with COVID-19 were assigned a placebo, anticoagulant or antiplatelet therapy to evaluate the impact on major cardiopulmonary outcomes within 45 days. Patients were randomized 1:1:1:1 to Aspirin 81mg daily, prophylactic-dose apixaban, therapeutic-dose apixaban, or placebo for 45 days with a primary end point that was a composite of all-cause mortality, symptomatic venous or arterial thromboembolism, myocardial infarction, stroke, or hospitalization for cardiovascular or pulmonary cause. The trial was stopped early because of an unanticipated low event rate. Among the 558 patients who initiated treatment, the primary composite end point occurred in 1 patient (0.7%) in the aspirin group, 1 patient (0.7%) in the 2.5-mg apixaban group, 2 patients (1.4%) in the 5-mg apixaban group, and 1 patient (0.7%) in the placebo group. In this trial, random allocation to aspirin or apixaban did not reduce rates of cardiopulmonary hospitalization compared with placebo.
CDC Morbidity and Mortality Weekly Reports (MMWR)
Vaccination reduces risk of COVID-19 hospitalization by 93% for adolescents age 12-18 years
In this test-negative, case-control study at 19 pediatric hospitals in 16 states during June 1–September 30, 2021, the effectiveness of the Pfizer-BioNTech vaccine against COVID-19 hospitalization was assessed among children and adolescents aged 12–18 years. Among 464 hospitalized persons aged 12–18 years (179 case-patients and 285 controls), the median age was 15 years, 72% had at least one underlying condition, including obesity, and 68% attended in-person school. Effectiveness of 2 doses of Pfizer-BioNTech vaccine against COVID-19 hospitalization was 93% (95% CI = 83%–97%), during the period when the Delta variant was the predominant variant. Case-patients more frequently resided in areas with higher social vulnerability index scores§§ (median = 0.67) than did controls (median = 0.58) (p = 0.02). Among 179 COVID-19 case-patients, six (3%) were vaccinated and 173 (97%) were unvaccinated. Overall, 77 (43%) case-patients were admitted to an intensive care unit, and 29 (16%) critically ill case-patients received life support during hospitalization, including invasive mechanical ventilation, vasoactive infusions, or extracorporeal membrane oxygenation; two of these 29 critically ill patients (7%) died. All 77 case-patients admitted to the intensive care unit, all 29 critically ill case-patients, and both deaths occurred among unvaccinated case-patients. Among 169 case-patients with available hospital discharge data, the median length of hospital stay was 5 days for unvaccinated case-patients and 3 days for vaccinated case-patients.
RECURRENT TOPICS
Providing COVID-19 vaccinations
In addition to the most recent CDC recommendation explained above, we still recommend that all healthcare providers outreach to their patients who are immunocompromised and are candidates for a third vaccine dose, whether they received Pfizer-BioNTech or Moderna.
All Alaskans and people who work or live in Alaska who are aged 12 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Pregnancy
On September 29, the CDC released a health advisory strongly recommending COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology.
Monoclonal Antibodies
Monoclonal antibody treatment for COVID-19, REGEN-COV (casirivimab and imdevimab) and Eli Lilly’s bamlanivimab and etesevimab, have been approved to treat mild-moderate COVID-19 and for post-exposure prophylaxis of COVID-19 in individuals age 12 years and older who are at high risk for progression to severe COVID-19.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the CDC webpage on Monoclonal Antibodies for High-Risk COVID-19 patients and COVID-19 Monoclonal Antibody Resources for Healthcare Providers.
Ivermectin
On August 26, the CDC issued a Health Advisory about the increase in ivermectin prescriptions and an associated rise in the number of calls to poison centers reporting overdoses or adverse effects.
A Cochrane Review published July 28 concluded, the “reliable evidence does not support the use of ivermectin for treatment or prevention of COVID‐19.” In addition, the FDA has recently created a webpage further explaining why you should not use ivermectin to treat or prevent COVID-19 and the potential harms of taking a veterinary formulation of this mediation. Infectious Disease Society of America (IDSA) guidelines DO NOT recommend ivermectin.
Post-acute Sequelae of COVID-19 (PASC)
More than half of COVID-19 survivors experienced PASC 6 months after recovery; most common sequelae involved functional mobility impairments, pulmonary abnormalities, and mental health disorders
In this systematic review of the short-term and long-term PASC, authors identified 57 studies with 250,351 survivors of COVID-19 who met inclusion criteria for having been diagnosed with COVID-19 and reported PASC frequencies. The median proportion of COVID-19 survivors experiencing at least 1 PASC at 1 month was 54.0%; at 2-5 months, 55.0%; and at 6 or more months, 54.0%. 5 of 10 survivors of COVID-19 developed a broad array of pulmonary and extrapulmonary clinical manifestations, including nervous system and neurocognitive disorders (ranging from 8-23%), mental health disorders (13.3-29.6%), cardiovascular disorders (9.3-13.3%), gastrointestinal disorders (6%), skin disorders (2.8%), and signs and symptoms related to poor general well-being, including malaise, fatigue, musculoskeletal pain, and reduced quality of life (10.0-37.5%).
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
Myocarditis
For the latest recommendations, check out the CDC webpage on myocarditis and COVID-19 vaccines
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 vaccines available in Alaska.
Aside from COVID-19
CDC and ACIP release recommendations for seasonal Influenza vaccination
Routine annual influenza vaccination is recommended for all persons aged ≥6 months who do not have contraindications. Influenza vaccine may be administered at the same time as COVID-19 vaccine. Detailed recommendations for influenza vaccination for persons currently infected with COVID-19 are available from CDC.
Approximately 2 million youths are current e-cigarette users.
A recent MMWR reviewed results of the 2021 National Youth Tobacco Survey which found that 11.3% of high schoolers and 2.8% of middle schoolers self-report current e-cigarette use. Most youth e-cigarette users consume flavored e-cigarettes with the most popular flavors of fruit or candy, desserts and other sweets.
DEA issues a Public Safety Alert on sharp increase in counterfeit pills containing fentanyl and meth.
The Drug Enforcement Administration issued a warning after identifying a dramatic rise in counterfeit pills containing lethal doses of fentanyl (at least 2 mcg per pill). In recent lab analyses at the DEA, 40% of seized pills contained a potentially lethal dose of fentanyl. Counterfeit pills have been seized in every U.S. state and are often sold on social media and e-commerce platforms. Additional information, including visual comparisons between authentic and counterfeit versions of common opiates, is available from DEA’s One Pill Can Kill campaign. This alert does NOT apply to prescribed medications dispensed by licensed pharmacists.
Upcoming Events/Conferences/Presentations
Free opioid prescribing education on October 26
On October 26 from 11am-2pm, the Division of Behavioral Health has partnered with Boston University School of Medicine to provide a free opioid prescribing education opportunity. This workshop is intended for physicians, nurse practitioners, registered nurses, physician assistants, nurses, dentists, pharmacists, and allied health professionals who manage acute and chronic pain. SCOPE of Pain is a series of continuing medical education/continuing nursing education activities designed to help you safely and effectively manage patients with acute and/or chronic pain, when appropriate, with opioid analgesics.
- Effective communication skills and the potential risks and benefits of opioids for managing acute and chronic pain
- The assessment of opioid misuse risk and recognition and treatment of opioid use disorder
- Helping you safely and effectively manage patients with acute and/or chronic pain, when appropriate, with opioid analgesics
Registration required at scopeofpain.org (select Core curriculum from the top menu, choose Live conferences, select the red button)
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule for the fall and the Zoom link.
10/22: Elisha Brownson, MD: Imaging Decisions in Pediatric Trauma
11/05: Rosalyn Singleton, MD: Respiratory/RSV/COVID Hospitalization trends and future interventions.
11/15: Mary Owen, MD: Tlingit People
11/19: Katie Presser, PharmD: Statewide Antimicrobial Stewardship
12/03: Marah Gotcsik, MD: ANMC Guideline on Preterm Infant Nutrition through 2 Years Old
12/10: Leslie Kerzner, MD: Care of the NICU Grad for Primary Care Providers
Join Zoom Meeting
https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One tap mobile
+16699006833,,98667611681#
Use of Valid Background Check Clearances by Multiple Employers
Providers who have applicants with pending background checks with DHSS BCU may allow individuals to start work prior to the Background Check Program completing their check IF the applicant has documented proof of having a current Alaska DHSS background check (provisional or complete) for another DHSS provider. The applicant must provide their new employer a copy of the final background check eligibility letter for the other provider, and providers are required to maintain a copy of that eligibly document in the employee’s file. Providers who hire employees in this manner MUST provide supervised access to those employees, i.e., to ensure the protection of recipients of services, the provider must maintain a prudent level of awareness of the whereabouts of an individual for whom supervised access is required. Employees working in this way may NOT be the only individual working in a facility or a setting, as another employee must be present to provide the supervised access. The provider’s oversight agency will monitor providers to ensure they are in compliance with these requirements, and providers must submit proof of compliance to those agencies upon request. Questions? Please contact your DHSS oversight division.
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
The most up-to-date, evidence based COVID-19 treatment guidelines can be found at:
IDSA Guidelines on the Treatment and Management of Patient with COVID-19
NIH COVID-19 Treatment Guidelines
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
AK Clinical Reminders — UPDATED October 20, 2021
COVID-19 testing guidelines and test site locator

These ECHO sessions are produced and facilitated by
UAA’s Center for Human Development Alaska ECHO project
in partnership with the State of Alaska, Department of Health & Social Services
Session information and recordings of previous ECHO sessions
subscribe to ECHO calendar updates | email: echo@alaskachd.org | website: akecho.org
Upcoming Session Highlights:
Special Pop-Up Session: Treatment for COVID-19
Thursday, October 21, 5:00-6:00 PM
This special pop-up is open to all Alaskans and will feature a presentation on Treatment for COVID-19 by the State of Alaska Department of Health and Social Services (DHSS) Public Health Team, followed by a public Q&A session. Register for this special session here. Questions may be submitted online prior to the pop-up.
Perinatal ECHO Session: Critical Congenital Heart Defects
Thursday, October 21, 6:00-7:00pm
Register
This session will feature a didactic presentation on critical congenital heart defects in Alaska by Dr. James Christiansen, pediatric cardiologist, and Chris Barnett, epidemiologist and program manager of the Alaska Birth Defects Registry. We will also have case presentations by pediatric cardiologists, Dr. Scott Wellmann and Dr. Kevin Kollins. As always, we will have ample time for Q&A and discussion with presenters and the hub team.
Regular Series
Alaska Medical Provider ECHO (formerly COVID-19 for AK Healthcare Providers)
Bi-monthly on the 1st and 3rd Tuesday of the month from 7-8 pm
This ECHO aims to increase knowledge and share best practices among medical providers across Alaska as well as to increase access to information for those living in rural areas of the state.
Register for our Alaska Medical Providers ECHO
School Health ECHO
Every Monday from 3:30-4:30 p.m Register
The School Health ECHO is a virtual learning network intended for professionals in the education setting (administrators, school-based nurses, etc.) to interface with a team of medical and education experts in Alaska.
Vaccine ECHO for Providers
Weekly on Tuesday from 2-3 p.m. Register
The Vaccine ECHO for providers provides planning and operation updates to vaccine providers across Alaska, while answering any questions you may have.
Palliative Care ECHO
Monthly on the first Tuesday from 12-1 p.m.
This monthly ECHO is for all Alaskan healthcare disciplines supporting patients with serious illness and aims to provide support and up-to-date information regarding Palliative Care during this period of COVID-19.
Public Science ECHO
Weekly on Wednesday from 12-1 p.m. register via Zoom
The Alaska Public Health Science ECHO is a virtual learning network intended for the general public to interface with our Public Health Leadership Team to explore the science of the COVID-19 virus, other public health topics, and current best practices. Or view via concurrent livestream to Facebook: https://www.facebook.com/akechoprograms
Local Government Public Health ECHO
Monthly on the third Wednesday from 3-4 p.m. Register
The Local Government Public Health Analysis ECHO is a virtual learning environment intended for local Alaska government leaders to interact with the State Public Health Leadership team and focuses on pandemic mitigation tools available, and how to use them.
Long Term Care Facilities ECHO
Second Wednesday of the month from 4-5 p.m. Register
Please join other staff and administrators of Alaska’s assisted living homes and residential care facilities to gather, learn, share, and grow. COVID has disrupted the fabric of our daily life and we can always learn from each other as we adjust to the new normal.
Healthcare Specific Situational Awareness ECHO
Weekly on Thursday from 12-1 p.m. Register
The Healthcare Specific Situational ECHO is a virtual learning network intended for healthcare professionals to interface with our Public Health Leadership Team to explore current best practices and the most recent information related to Public Health.
Perinatal ECHO
Monthly on 3rd Thursday from 6-7 p.m. Register
The Alaska Perinatal ECHO is a virtual learning network intended for medical providers caring for pregnant patients and their newborns.
EMS ECHO
Monthly on the 1st and 3rd Wednesday 1-2 p.m Register
The EMS ECHO is a virtual learning network intended for Emergency Medical Services and related personnel in Alaska to amplify best practices. Sessions are topic-driven and typically include a guest presenter or a brief lecture with an interactive case or process discussion.
AK COVID-19 clinical hotline for physicians: 833-751-4212. Staffed 24/7.
8PM-8AM is for urgent/emergent questions only.
AK Responders Relief Line: 24/7 behavioral health for everyone working in healthcare
during the COVID-19 pandemic: 1-844-985-8275
|
|
