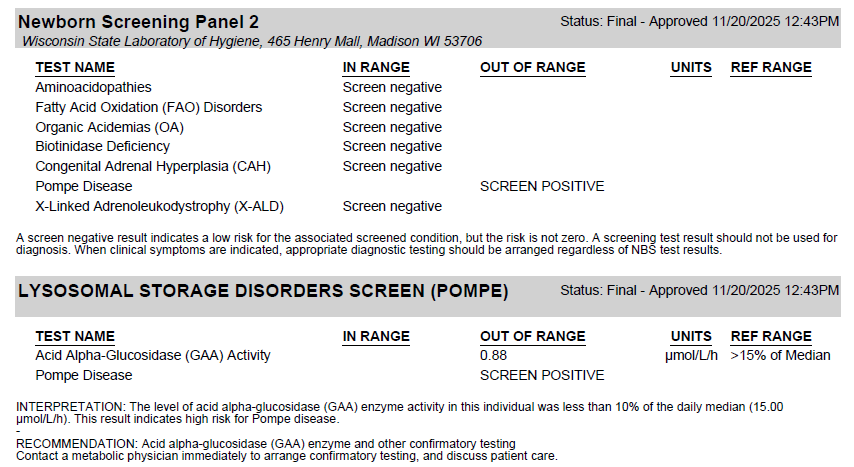
Following the Montana Newborn Screening Advisory Committee's recommendation, the Montana Public Health Laboratory (MTPHL) will be adding Pompe disease to the Montana newborn screening panel. Testing will be conducted at the Wisconsin State Lab of Hygiene beginning on January 15, 2026. Pompe disease will be reported as Screen Negative, Screen Positive, or Inconclusive.
Sample report:
More Information:
Pompe disease is a type of glycogen storage disease, a genetic condition in which a complex sugar called glycogen builds up in your body’s cells. The disease results from a deficiency of the digestive enzyme acid alpha-glucosidase (GAA). GAA typically breaks down complex sugars in your body. A lack of the GAA enzyme causes a glycogen buildup within the body’s organ cells, causing breakdown, especially in the heart and skeletal muscles. In the United States, Pompe disease affects about 1 in every 40,000 individuals. Two main types of Pompe disease differ based on age of onset and severity. These types include infantile-onset and late-onset (juvenile or adult-onset). Infantile-onset is the most severe form of the disease and is caused by complete or very little absence of the GAA enzyme. Symptoms of this form most often start around 4 months of age. Symptoms include poor muscle tone, delays or respiratory symptoms due to heart failure, enlarged tongues and livers, and a protruding abdomen. Without treatment, death often occurs in one to two years of age.
Late-onset Pompe disease can appear at any age but is distinguished from infantile-onset Pompe disease by the absence of an enlarged heart. Individuals with this type have a reduced amount of the GAA enzyme and often present with a milder, slower progression of the disease; however, the younger the age of onset, the more severe the symptoms. These symptoms include muscle weakness that leads to breathing issues, and without treatment, these individuals usually succumb to respiratory complications. Heart complications are absent in this form of the disease.
Pompe disease is diagnosed using several methods, including physical exams and blood tests. Specific tests include heart studies, such as an electrocardiogram (EKG) or an echocardiogram; pulmonary function tests that measure lung capacity and breathing; muscle tests that measure muscle function; and sleep studies. Lab tests include bloodspot tests, urine glucotetrasaccharide (HEX4), GAA DNA testing, and cross-reactive immunologic material (CRIM) test status. A bloodspot test for Pompe disease uses the creatine:creatinine ratio, then divides it by the GAA activity. This ratio can differentiate true cases of infantile and late-onset Pompe disease from false-positive cases, such as carrier states and GAA enzyme pseudodeficiency.
Treatment for Pompe disease includes enzyme replacement therapy (ERT) with genetically engineered medications that help decrease heart size, maintain normal heart function, improve muscle function, and reduce glycogen buildup. The U.S. Food and Drug Administration (FDA) approved treatments for infantile Pompe disease include Lumizyme and the two-component therapy for adults with late-onset Pompe disease, Pombiliti (cipaglucosidase alfa-atga) and Opfolda (miglustat).
Pompe disease is included on the Recommended Uniform Screening Panel (RUSP), the national guideline for newborn screening—currently, 45 states screen for Pompe disease.
Please follow this link for follow-up testing for Pompe: