Outdoor Exercise and Asthma
Summertime in Montana allows for ample opportunities to get outdoor exercise, however, this can present some challenges for your patients with asthma. According to the American Academy of Allergy, Asthma and Immunology, exercise-induced bronchoconstriction (EIB) can cause asthma symptoms (e.g., shortness of breath, chest tightness, wheezing or coughing) upon exercise or during other activities that require physical exertion. Patients with EIB only experience asthma symptoms with exercise while others with chronic asthma may find exercise is a trigger for their disease. In either case, it may be appropriate for your patient to pre-treat with their short acting bronchodilator (SABA) inhaler 15 minutes prior to physical activity to help open their airways.

Some common outdoor activities which may exacerbate asthma include running, hiking/backpacking, swimming, and outdoor sports (e.g., softball, soccer). Activities that require endurance tend to exacerbate symptoms more compared to those that require short bursts of energy. Warm weather activities are less likely to cause asthma symptoms. Additionally, chemicals used in a swimming pool can be a trigger in addition to exercise. It is important to reduce other asthma triggers such as seasonal allergies because they can worsen EIB. Giving patients with EIB the tools to successfully exercise outdoors can help them reduce asthma exacerbations and maintain healthy activity levels.
|
Recommended Pharmacist Actions and Counseling Points:
*Make sure patients with chronic asthma or EIB:
- Have a SABA inhaler that is not expired
- Keep their SABA inhaler on them while exercising outdoors or participating in outdoor recreation such as hiking or camping
- If appropriate, use their SABA inhaler 15 minutes before exercise
- Have an asthma action plan to follow
- Implement warm up and cool down periods before and after exercise
- Stay hydrated
- Avoid exercising when ill
- Remain adherent to any controller medications for asthma
*Help patients control additional triggers such as seasonal allergies and poor air quality by:
- Recommending OTC allergy medications when appropriate
- Use air quality index (AQI) information to avoid outdoor exposure during high pollen count or unhealthy air days
Written by Jade Bosic-Reiniger, PharmD, MPH, BC-ADM, AE-C
Pharmacists Call To Action: Suboptimal Use of Proven Therapies in Type 2 Diabetes
Type 2 Diabetes and Atherosclerotic Cardiovascular Disease (ASCVD)
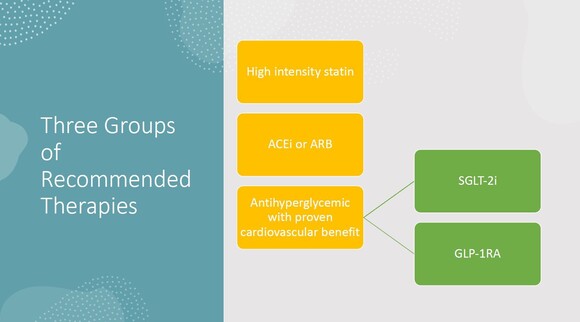
The American Diabetes Association 2023 guidelines for pharmacologic management of people with type 2 diabetes and existing ASCVD include high intensity statin, ACE inhibitor or ARB, and SGLT-2 inhibitor and/or GLP-1 receptor agonist therapy for cardiovascular event risk reduction.
What percentage of eligible patients are receiving these medications?
Numerous studies have indicated that the initiation rate of the newer medication classes (SGLT-2i and GLP-1 RA) has been lower than expected. The use of older medications is higher but still suboptimal. According to this JAMA network article from 2022, examining guideline directed therapies in people with type 2 diabetes and ASCVD, 58.6% were on statins, 28.6% on a high intensity statin, 45.5% were on ACE/ARBs, 3.9% on GLP-1 RA, and 2.8% on SGLT-2i.
Coordinate-Diabetes Study: Clinical inertia in cardiology clinics.
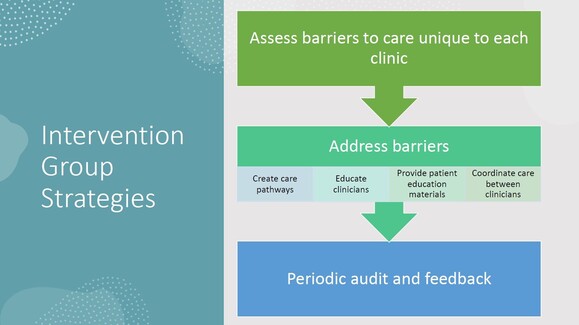
Most people with type 2 diabetes and ASCVD are seen by primary care providers, but the second most visited providers are cardiologists. In this study of prescribing habits in cardiovascular clinics, looking at people with type 2 diabetes and ASCVD, only 2.7% were on all three and 37.4% were on none of the recommended therapies. The Coordinate-Diabetes study was designed to assess the change in usage of three groups of medication therapies in people with type 2 diabetes and ASCVD in 42 cardiology clinics after a designed intervention. The primary outcome was the change in usage after 12 months in the intervention group.
 Results and conclusions:
After 12 months (6 months for some due to COVID-19 interference) use of the three recommended medication groups in the intervention group increased to 37.9% vs 14.5% in the usual care group. The study shows that a purposeful and well-designed effort can increase the use of guideline directed therapy. It is unrealistic to think of a 100% utilization rate but certainly we can do better for our patients with type 2 diabetes and ASCVD. The authors suggest that team-based care should include other professions including pharmacists.
 3MinuteExtraMile suggested action steps:
- Pharmacists involved in medication therapy management can look at prescription records, identify people with suboptimal therapy and make suggestions.
- We can develop talking points on the advantages of the medications and clarify misconceptions.
- Pharmacists can help people navigate the issues of cost with the newer agents.
- Look at the Coordinate-Diabetes website for tools and resources that might be helpful in talking to patients.
- Check out the American Diabetes Association's website on its initiative to overcome therapeutic inertia. Great resources and guidance are available there as well.
James Bennett BsPharm, BCGP, CDCES
Bozeman, MT
Please share with colleagues and encourage them to Click to subscribe
|

