|
Management of Hyperglycemia in Type 2 Diabetes:
An Updated Consensus Statement
The American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) first published the consensus statement, Management of Hyperglycemia in Type 2 Diabetes, in 2006. The most recent update is available in the November, 2022, issue of Diabetes Care.
How does this document differ from the ADA Standards of Care?
This consensus statement looks only at type 2 diabetes and offers specific guidance for use of pharmacologic therapies. In addition, and in concise language, it touches on other elements of care including:
- Social Determinants of Health
- Importance of weight loss
- Physical activity, dietary quality, and healthy sleep patterns
- Diabetes Self-management Education and Support
- Therapeutic inertia
Back to glycemic control
The cardiorenal effects of the SGLT-2i and GLP-1 RA medication classes have, in some ways, dominated the diabetes news lately. This document reminds us of the importance of early and aggressive treatment to reach glycemic targets, especially in younger people or those with longer life expectancies to reduce microvascular and macrovascular* effects.
*The effect of glycemic control on macrovascular complications is less well defined but supported by epidemiological data and meta-analyses.
A focus on weight reduction
According to the authors, weight loss of 5-15% should be considered a primary target for many people with type 2 diabetes. Current information suggests that weight loss of 5-10% improves metabolic parameters, and weight loss of 10-15% has disease modifying effects that can result in diabetes remission.
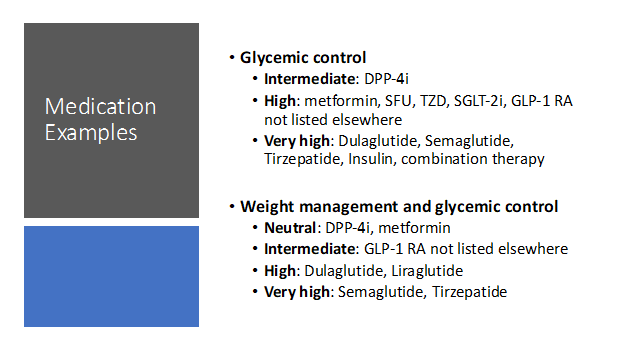
Key points in choosing glucose lowering medications
- Contrary to some of the talk we hear these days, metformin is not dead yet.
- Choose medications that provide efficacy needed to reach goals.
- Glucose lowering ability for recommended medications is categorized as intermediate, high, and very high.
- Efficacy for agents that lower blood glucose and achieve weight loss are listed as neutral, intermediate, high, and very high.
This consensus statement is an excellent reference, addressing type 2 diabetes patient care in a holistic and patient centered manner. Pharmacists will be interested in the section called “Choice of Glucose-Lowering Medication”. It covers medication classes by looking at current data and explaining the reasons for using or not using each class of medication in a particular situation. There are practical tips for clinicians after each section. See below for some patient talking points and clinical pearls.
3 minute EXTRA mile: clinical pearls for GLP-1 RA and GLP-1/GIP RA therapies.
- Enable weight loss that improves cardiovascular risk profile and lowers A1c
- Weight loss is significant, for example tirzepatide at the 15 mg per week dose can produce 20% weight reduction
- Should be used as the first injectable before insulin
- Added to basal insulin can preclude the need for prandial insulin and result in lowering doses or eliminating of SFUs and or DPP-4 inhibitors. This also reduces risk of hypoglycemia
- Used alone do not cause hypoglycemia
- Avoiding the main adverse events, nausea, vomiting, diarrhea
- Eat slowly and mindfully
- Avoid high fat meals
- Be aware of the feeling of fullness and stop eating at that point
- Nausea, if it occurs, usually goes away within the first two weeks
- Start with the lowest dose and titrate over time to the optimal dose
Abbreviations: dipeptidyl peptidase-4 inhibitors (DPP-4i), sodium-glucose cotransporter 2 inhibitor (SGLT2i), glucagon-like-peptide-1 receptor agonist (GLP-1 RA), thiazolidinedione (TZD), sulfonylurea (SFU), glucose-dependent insulinotropic polypeptide (GIP)
James Bennett BsPharm, CDCES, BCGP
Bozeman, Montana
SAMAs and LAMAs
A variety of short and long-acting muscarinic antagonists or anticholinergic agents are available for treating both COPD and asthma. Competitive inhibition of muscarinic receptor subtypes M1, M2, and M3 in mucus glands and bronchial smooth muscle yields bronchodilation or relaxing of the muscles. Long-acting antimuscarinics (tiotropium, umeclidinium, aclidinium, glycopyrrolate) are more selective to the M3 receptor subtype and dissociate more slowly than the short-acting ipratropium. Long-acting muscarinic antagonists (LAMAs) can be used as maintenance therapy for COPD or asthma, but none should be used for acute relief of asthma or COPD-related symptoms.
 |
|
According to the EPR 2020 update, LAMAs are not recommended for asthma treatment until step 3, as an alternative therapy for those ≥ 12 years of age and should always be paired with an inhaled corticosteroid (ICS). Combination therapy with an ICS-LABA plus LAMA is preferred for those with persistent asthma in step 5 of therapy. An inhaler approved for both asthma and COPD with this combination is Trelegy (fluticasone furoate, umeclidinium, and vilanterol) where Breztri (budesonide, glycopyrrolate, and formoterol fumarate) is only approved for use in COPD.
|
No short-acting muscarinic antagonist (SAMA) is recommended for treating asthma, according to the EPR guidelines. Proper administration of any anticholinergic can improve lung function, reduce exacerbations, and improve patient outcomes for most with COPD or asthma.
Pharmacist Action Steps:
- Counsel patients on the commonly associated side effects of antimuscarinic agents; dry mouth, constipation, runny or stuffy nose, and headache. These medications may also cause dizziness, blurred vision, or a metallic taste.
- Monitor patients who are taking antimuscarinics and have renal dysfunction (CrCl ≤60 mL/min), as anticholinergic effects may be more apparent.
- Identify causes for previously failed therapies for patients with asthma (such as adherence, cost, or side effects) and where improvements may be warranted, other than a medication change.
- Discuss adherence with patients who have difficulties remembering to take their maintenance medication.
Written by Tristan Egelhoff, Pharm D Candidate. Reviewed by Rachael Zins, PharmD, AE-C
Please share with colleagues and encourage them to Click to subscribe
|

