COVID-19 Alaska Clinical Update
Wednesday, August 11, 2021
Major companies mandating COVID-19 vaccination
Some of the largest employers in the US recently have announced SARS-CoV-2 vaccination mandates for all or some of their employees amid a surge of COVID-19 cases. Walmart, Disney, Google, Tyson Foods, Delta and United Airlines, and Goldman Sachs are just some of the companies that are requiring that at least some of their employees be vaccinated, either as a condition of employment or in order to return to corporate office buildings.
The US Equal Employment Opportunity Commission (EEOC) has issued guidance generally permitting employers to institute vaccination mandates in the workplace as long as reasonable accommodations are offered to those with religious beliefs, disabilities, or other conditions that might prohibit vaccination. On July 6, the US Department of Justice published a memorandum explaining that Section 564 of the Food, Drug, and Cosmetic Act, which authorizes the US FDA to issue emergency use authorization (EUA), does not prohibit public and private entities such as businesses and schools from imposing SARS-CoV-2 vaccine requirements. In essence, the regulation permits employers to implement policies requiring vaccination as a condition of employment even when the vaccine is being used under an EUA.
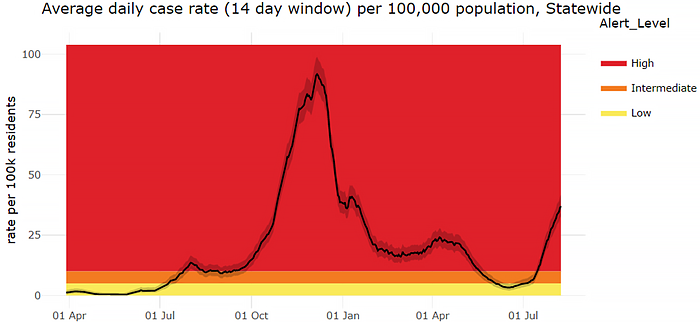
Alaska changes alert level system to align with CDC’s levels of transmission
On Monday, Aug. 9, DHSS will make changes to the alert level system which is used to inform communities about what COVID-19 looks like in their area. These changes to Alaska’s alert system will: better align with CDC’s levels of transmission, make it more sensitive to recent changes in the number of reported COVID-19 cases, and provide more locally relevant information. Key changes include:
- Moving from three alert levels to four levels:
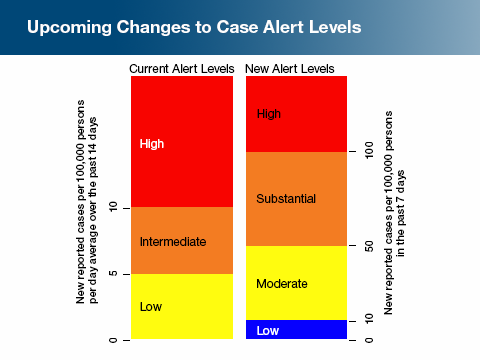
- Changing the calculation used from the average number of reported cases per 100,000 people over the past 14 days to the reported number of cases per 100,000 people over the past 7 days
- Calculating alert levels for all boroughs and census areas with a population of over 1,000. Those areas with less than 1,000 people will be combined with a neighboring geographic area.
In critically ill COVID-19 patients, therapeutic-dose anticoagulation with heparin did not result in greater probability of survival than did usual-care thromboprophylaxis
Thrombosis and inflammation may contribute to morbidity and mortality among patients with severe COVID-19 infection. In this open-label adaptive randomized control trial, 1098 patients receiving ICU-level care for COVID-19 illness were randomized to receive either an initial strategy of therapeutic-dose anticoagulation with heparin or usual-care pharmacologic thromboprophylaxis. The primary outcome was organ support-free days (meaning the patient did not require high-flow nasal cannula, noninvasive or invasive ventilation, ECMO, vasopressors, or inotropes) and the and secondary outcomes were survival to hospital discharge, major thrombotic events or death, and any thrombotic event or death. There was no significant difference in organ support-free days or survival to hospital discharge. A major bleeding event occurred during the treatment period in 3.8% of the patients assigned to receive therapeutic-dose anticoagulation and in 2.3% of those assigned to receive usual-care thromboprophylaxis.
Researchers predict high likelihood of emergence of vaccine-resistant variant
In separate reports, groups of researchers from both Austria and the UK warn of the near inevitability of the emergence of vaccine-resistant variants of the SARS-CoV-2 virus. The reports claim that the highest risk of vaccine-resistant strain establishment occurs when a large proportion of the population is vaccinated but viral transmission is high, underlining the importance of controlling transmission through public health interventions while continuing vaccination campaigns. The Austrian report says “the emergence of a partially or fully vaccine-resistant strain and its eventual establishment appears inevitable.”
Risk of thrombosis with thrombocytopenia syndrome following AstraZeneca vaccination ranges from 8.1 to 2.3 per million doses
In this peer reviewed analysis of cases of thrombosis with thrombocytopenia syndrome (TTS) following AstraZeneca-Oxford COVID-19 vaccination, researchers identified 399 cases of TTS among 49.2 million individuals who received the first dose of the vaccine, equating to an estimated risk of 8.1 cases per million doses. The risk decreased following the second dose, down to 2.3 per million doses—13 cases of TTS among 5.62 million individuals who received the second dose. The researchers estimated that the average over a 14-day period prior to the pandemic was as high as 7.16 cases of TTS per million people. The AstraZeneca-Oxford vaccine has not been authorized for use in the United States, however it shares a similar mechanism to the Johnson & Johnson-Janssen vaccine.
Pfizer-BioNTech COVID-19 composite vaccine efficacy for six months is approximately 91%; vaccine efficacy appears to wane approximately 6% every 2 months
The placebo-controlled efficacy trial included nearly 45,000 participants aged 16 and older, and roughly 2,250 participants between the ages of 12 and 15. According to the study, the vaccine’s composite efficacy through 6 months was 91% among evaluable participants and irrespective of previous SARS-CoV-2 infection. Vaccine efficacy against severe disease was 97%. From 7 days to <2 months post-dose 2, vaccine efficacy (VE) was 96.2% (95% CI [93.3-98.1]); from 2 months to <4 months, VE was 90.1% (95% CI [86.6-92.9]); and from 4 months to the data cut-off, VE was 83.7% (95% CI [74.7-89.9]). In South Africa, where the SARS-CoV-2 Beta variant (B.1.351) was dominant during the study, the vaccine efficacy was 100%. However, the study did not evaluate vaccine efficacy against the now widespread Delta variant, and the company acknowledged that additional research is necessary to fully evaluate the vaccine against new variants.
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
FDA approval for COVID-19 vaccines anticipated in early autumn
Pfizer-BioNTech applied to the FA for full approval of its COVID-19 mRNA vaccine on May 7, 2021. President Biden has said that he expects full approval for the vaccine in early fall but according to the New York Times, the FDA’s unofficial deadline is by September 6 or sooner.
Some countries are recommending a third “booster” shot for mRNA COVID vaccines
On July 29, Israel became the first country to approve third doses of the Pfizer-BioNTech vaccine for people ages 60 and older who are at least 5 months post-second dose. Israel already recommended a booster shot for immunocompromised individuals. France and Germany have announced their intention to give boosters to the elderly, immunocompromised, and nursing home residents beginning in September.
CDC Morbidity and Mortality Weekly Reports
Unvaccinated individuals have more than double the risk of reinfection compared to those who are vaccinated
In this case-control study of Kentucky residents infected with SARS-CoV-2 in 2020, vaccination status of those reinfected during May–June 2021 was compared with that of residents who were not reinfected. Being unvaccinated was associated with 2.34 times the odds of reinfection compared with being fully vaccinated. Overall, 246 case-patients were successfully matched by age, sex, and date of initial infection with 492 controls. Among the population included in the analysis, 60.6% were female, and 204 (82.9%) case-patients were initially infected during October–December 2020. Kentucky residents with previous infections who were unvaccinated had 2.34 times the odds of reinfection (OR = 2.34; 95% CI = 1.58–3.47) compared with those who were fully vaccinated; partial vaccination was not significantly associated with reinfection (OR = 1.56; 95% CI = 0.81–3.01).
From February-April 2021, COVID-19 vaccines were 84-96% effective at preventing hospitalization due to COVID-19 infection
To determine the real-world effectiveness of the three currently authorized COVID-19 vaccines among persons aged ≥65 years during February 1–April 30, 2021, data on 7,280 patients from 14 states were analyzed. Among adults aged 65–74 years, effectiveness of full vaccination in preventing COVID-19–associated hospitalization was 96% (95% confidence interval [CI] = 94%–98%) for Pfizer-BioNTech, 96% (95% CI = 95%–98%) for Moderna, and 84% (95% CI = 64%–93%) for Johnson & Johnson-Janssen vaccine products. Effectiveness of full vaccination in preventing COVID-19–associated hospitalization among adults aged ≥75 years was 91% (95% CI = 87%–94%) for Pfizer-BioNTech, 96% (95% CI = 93%–98%) for Moderna, and 85% (95% CI = 72%–92%) for Johnson & Johnson-Janssen vaccine products. COVID-19 vaccines currently authorized in the United States are highly effective in preventing COVID-19–associated hospitalizations in older adults. One major limitation is the study period for this analysis occurred before the predominance of the B.1.617.2 (Delta) variant; changes in circulating SARS-CoV-2 variants might affect vaccine effectiveness when assessed over time.
RECURRENT TOPICS
Monoclonal Antibodies
Prophylactic treatment with monoclonal antibodies reduced risk of symptomatic COVID-19 by 81.4%
In this industry sponsored randomized control trial, 1505 participants were enrolled within 96 hours after a household contact received a diagnosis of SARS-CoV-2 infection to receive Regeneron’s monoclonal antibody therapy (REGEN-COV) or matching placebo administered by means of subcutaneous injection. Symptomatic SARS-CoV-2 infection developed in 11 of 753 participants in the REGEN-COV group (1.5%) and in 59 of 752 participants in the placebo group (7.8%) (relative risk reduction 81.4%). In weeks 2 to 4, a total of 2 of 753 participants in the REGEN-COV group (0.3%) and 27 of 752 participants in the placebo group (3.6%) had symptomatic SARS-CoV-2 infection (relative risk reduction, 92.6%). REGEN-COV also prevented symptomatic and asymptomatic infections overall (relative risk reduction, 66.4%). Among symptomatic infected participants, the median time to resolution of symptoms was 2 weeks shorter with REGEN-COV than with placebo (1.2 weeks and 3.2 weeks, respectively).
For the latest recommendations, check out the CDC webpage on Monoclonal Antibodies for High-Risk COVID-19 patients and COVID-19 Resources for Healthcare Providers.
Post-acute Sequelae of COVID-19 (PASC)
PASC in children is possible but less common than in adults
In this prospective cohort study from the UK, researchers followed 1734 children aged 5-17 years who had a positive SARS-CoV-2 test and calculable illness duration between September 2020 – January 2021 to determine prevalence of PASC in children. Data for the patients were reported by an adult proxy through a mobile app; more than 250,000 children were included in the database but only 1734 had confirmed test results and clear illness duration during the study period. The most common symptoms were headache and fatigue with symptoms lasting longer for older children than younger children. 4.4% of children (77 of 1734) had illness duration of at least 28 days, more commonly in older children than younger children with most common symptoms being fatigue, headache, and anosmia. 1.8% of children (25 of 1379) experienced symptoms for at least 56 days.
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
Myocarditis
For more information, check out the CDC webpage on myocarditis and COVID-19 vaccines
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 vaccines available in Alaska.
Aside from COVID-19
Alaska’s second annual Improving Diagnostic Accuracy in Medicine Virtual Conference will take place on September 6th and 7th. The conference includes keynote presentations, case studies, and patient stories to bring healthcare professionals together to learn with a unified goal of improving the care of all Alaskans.
CDC Clinical Support
There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by
to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
All Alaskans and people who work or live in Alaska who are aged 12 years and older are eligible for vaccination against COVID-19. Appointments can be made at covidvax.alaska.gov.
|
