Powassan Virus Activity in Wisconsin and Recommendations for Testing and Diagnosis
This message is being sent to the health alert network, local public health officers, Tribal health directors, local public health department nurses, local public health department staff, and infection preventionists.
Summary
As of June 2025, three cases of Powassan virus (POWV) disease have been reported in adult Wisconsin residents. All three individuals were hospitalized, and one died from the infection. In 2024, 12 cases of POWV disease were reported in Wisconsin residents, the highest number of cases reported in the state in a calendar year and the second most cases in the United States after Minnesota, which reported 14 cases last year. POWV is a tickborne virus spread by the blacklegged (deer) tick, the same tick that spreads Lyme disease, anaplasmosis, and several other diseases in Wisconsin. POWV infection can cause a mild febrile illness or neurologic disease that often presents as meningitis or encephalitis. Diagnosis of POWV disease can be delayed due to nonspecific symptomology, limited commercial laboratory testing, and lack of provider awareness.
The Wisconsin Department of Health Services (DHS) recommends that health care providers:
-
Consider POWV disease in patients with unexplained neurologic disease with known or possible tick exposure one to five weeks before illness onset.
- Order the appropriate diagnostic testing for patients with suspected POWV disease.
- POWV IgM testing in serum or cerebrospinal fluid (CSF), or
- POWV IgM in serum or CSF and POWV RT-PCR in whole blood, serum, or CSF, which may be particularly helpful for immunocompromised patients.
- Ensure timely reporting of POWV infections to state or local public health authorities.
- Promote tick bite prevention measures among individuals who spend time working or recreating outdoors, especially in the northern half of Wisconsin.
Background
POWV is a tickborne flavivirus that is transmitted to people by the bite of an infected blacklegged (deer) tick, Ixodes scapularis. Ticks become infected when they take a blood meal from an infected groundhog, skunk, squirrel, mouse, or other rodent. It is unknown exactly how long a tick must be attached to a person for POWV transmission to occur, but it is likely less than 12 hours and could be as little as 15 minutes. POWV can rarely be transmitted through blood transfusion.
POWV is rare, but there has been an increase in the number of cases reported in recent years. This increase could be from more people becoming infected with POWV, improvements in testing and diagnosis, or some combination of both. POWV disease can be prevented by taking measures to avoid tick bites.
Powassan surveillance
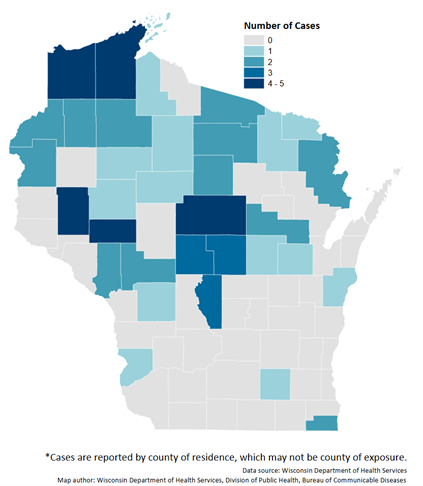
The first case of POWV disease in Wisconsin was identified in 2003. From 2003 through 2024, a total of 68 cases of POWV disease have been reported to public health. Public health surveillance for POWV disease is more likely to detect severe clinical cases, so it’s possible that mild febrile cases are significantly underreported. Cases of POWV disease are more common in the northern half of Wisconsin, where the blacklegged (deer) tick is more abundant (Figure 1). Nationally, cases of POWV disease are most common in the Upper Midwest and Northeast.
Figure 1: Powassan Virus Cases in Wisconsin (2003–2024)
 Clinical presentation
POWV can cause asymptomatic infection, non-specific febrile illness, or severe neurologic disease. Initial symptoms commonly include fever, headache, vomiting, and generalized weakness. The disease can progress to encephalitis, meningoencephalitis, or aseptic meningitis. Risk factors for neurologic disease include immunocompromising conditions or immunosuppressive medications, old age (≥60 years), and very young age (<10 years). Approximately 10% of patients with neurologic POWV disease die from the infection, and about 50% of patients who survive experience long term neurologic sequalae.
Symptoms of encephalitis can include altered mental status, seizures, speech problems (aphasia, dysarthria), paresis or paralysis, movement disorders, and cranial nerve palsies. Symptoms of meningitis can include severe headache, nuchal rigidity, photophobia, nausea, and vomiting.
CSF findings typically include lymphocytic pleocytosis in patients with encephalitis or meningitis, with neutrophils predominating early in the disease course. CSF protein is usually normal or mildly elevated, and glucose concentration is normal.
Other causes of encephalitis and aseptic meningitis should also be considered, as appropriate (for example, herpes simplex viruses, enteroviruses, West Nile virus (WNV), La Crosse virus (LACV), and Eastern equine encephalitis virus (EEEV)).
Testing recommendations
Which patients should be tested for POWV?
Testing for POWV infection is recommended for patients with symptoms of POWV disease, especially neurologic symptoms that cannot be explained by another etiology, and who have known or possible tick exposure one to five weeks prior to illness onset. Providers should be aware that ticks can be active in Wisconsin anytime temperatures are above 40° Fahrenheit, including during winter months.
Testing for POWV infection is not recommended in asymptomatic individuals, including asymptomatic individuals with a known tick bite. Febrile patients with possible tick exposure should also be tested for other more common tickborne illnesses, such as Lyme disease, anaplasmosis, ehrlichiosis, and babesiosis as these diseases are treatable.
POWV is one of several arboviruses transmitted in Wisconsin that can cause neurologic disease and the only one transmitted by ticks. Other arboviruses include WNV, Jamestown Canyon virus (JCV), LACV, and EEEV, which are transmitted by mosquitoes. DHS recommends that patients suspected of having any arboviral disease, such as POWV, also be tested for other circulating arboviruses since clinical features of these diseases overlap.
What tests should be ordered?
Patients suspected of having POWV disease should be tested using:
- POWV IgM antibody test, or
- POWV IgM antibody test and POWV RT-PCR (for immunocompromised patients).
Serology
Serologic testing is the primary method for diagnosing POWV. Initial testing can be performed using POWV IgM antibody testing in serum or in CSF for patients with neurologic disease. Due to the possibility of cross-reactivity between other flaviviruses, such as WNV, positive POWV IgM test results should be confirmed by neutralizing antibody testing (plaque-reduction neutralization test or PRNT) at CDC (Centers for Disease Control and Prevention). IgM antibodies are usually detectable during the first week of illness. If specimen is collected within eight days of illness onset, a negative IgM result does not rule out infection and repeat testing on a later specimen may be needed.
POWV IgM test availability:
-
POWV IgM antibody testing is available commercially at Mayo Clinic Laboratories. Mayo Clinic Laboratories provides more information about specimen collection, submission, and POWV IgM test performance.
- POWV IgM antibody testing is also available at the Wisconsin State Laboratory of Hygiene (WSLH). POWV IgM can be ordered alone (test code SS02251) or as part of an arbovirus IgM antibody panel (test code SS02201). No prior approval from DHS is required. The arbovirus IgM antibody panel includes IgM antibody tests for POWV, WNV, St. Louis encephalitis virus, LACV, JCV, and EEEV. Positive POWV IgM specimens are automatically reflexed to PRNT at CDC.
Molecular testing
Patients who are immunocompromised may have prolonged viremia and delayed antibody response. Therefore, immunocompromised patients may require molecular testing, such as RT-PCR, for diagnosis. A positive POWV RT-PCR result can confirm an acute infection; a negative POWV RT-PCR result, however, does not rule out infection. It is recommended that IgM testing is ordered together with RT-PCR testing.
POWV RT-PCR availability:
-
POWV RT-PCR testing is available commercially at Mayo Clinic Laboratories. More information about specimen type, collection, submission, and POWV RT-PCR test performance is available:
- POWV RT-PCR testing can also be performed at CDC on specimens from immunocompromised patients. To request POWV RT-PCR testing at CDC, please contact DHS, Bureau of Communicable Diseases at 608-267-9003 or dhsdphbcd@dhs.wisconsin.gov.
For additional information about when and how to order POWV testing through WSLH or CDC, providers can contact:
- DHS, Bureau of Communicable Diseases at 608-267-9003 or dhsdphbcd@dhs.wisconsin.gov, or
- WSLH Customer Service at 800-862-1013
Clinical management
There is no specific treatment for POWV disease. Clinical management is supportive. Patients with severe meningeal symptoms often require pain control for headaches and antiemetic therapy and rehydration for associated nausea and vomiting. Patients with encephalitis require close monitoring for the development of elevated intracranial pressure, seizures, and inability to protect their airway.
Prevention
No POWV vaccines are available for use in humans. In the absence of a vaccine, prevention of POWV infection depends on personal protective measures to decrease exposure to infected ticks. This includes avoiding wooded and bushy areas with high grass in endemic areas, using repellents to discourage tick attachment, and finding and removing ticks before they have a chance to attach. More information about reducing exposure to ticks is available on the DHS Tick Bite Prevention webpage and the CDC Preventing Tick Bites webpage.
POWV can rarely be transmitted through blood transfusion. People with confirmed POWV infection should not donate blood for 120 days (4 months) after their illness. POWV infections temporally associated with blood transfusion should be reported promptly to state or local public health authorities.
Resources
|

