
This update is being sent to members of the Wisconsin Travel Health Network.
Global Health Update
Cases of meningococcal disease associated with travel to Saudi Arabia
On June 6, 2024, the Centers for Disease Control and Prevention (CDC) released a Morbidity and Mortality Weekly Report (MMWR) providing details on recent cases of meningococcal disease associated with travel to Saudi Arabia as well as travel health recommendations for people visiting the country.
Investigation details
Twelve cases of invasive meningococcal disease (IMD) were identified in three countries including the United States (five), France (four) and United Kingdom (three). Of the 12 total cases identified, 10 occurred in adults aged 25 years and older and two cases occurred in children aged 0–12 years. The 10 adult case patients had all reported recent travel to Saudi Arabia and the two child patients were household contacts of an adult traveler. All travelers visited Saudi Arabia during March–May 2024, and symptom onset occurred upon return to their country of origin in April and May.
Travel recommendations
Travelers who are going to Saudi Arabia, should be up to date on all routine vaccines and travel related vaccines, including meningococcal vaccine. Additional information about health recommendations for travel to Saudi Arabia can be found on the CDC Traveler Health web page.
New Resource Available!
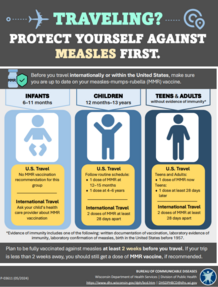
The Wisconsin Department of Health Services (DHS) Immunization Program recently published an updated resource on measles vaccination recommendations prior to travel. This informational handout is available in both English and Spanish and is a great resource for travel health providers!
This resource is available to download at the following links:
|
Obtaining Immunization Records for Travel
Finding old immunization information can be difficult and time-consuming. Therefore, it is critical that travelers keep an accurate and up-to-date record of the vaccinations they have received. Keeping an immunization record and storing it with other important documents (or in a safe place) will save travelers time and unnecessary hassle.
Travelers can ask their doctor, pharmacist or other vaccine provider for an immunization record form or download and use this form. They can then bring this record with them to health visits and ask their vaccine provider to sign and date the form for each vaccine they receive. That way, they can be sure that the immunization information is current and correct.
In Wisconsin, this information is added to the Wisconsin Immunization Registry (WIR). WIR is an online database that tracks vaccine records for Wisconsin children and adults. Travelers can access the WIR to look up their own immunization record. If they are a parent or legal guardian, they can also look up their children’s records. Many people in Wisconsin receive vaccines from more than one provider. Public access to WIR allows travelers to find their vaccine record quickly and easily, from anywhere they have access to a computer or smart phone.
Using the Wisconsin Immunization Registry
If travelers need to use WIR to look up vaccine records for themselves or a family member prior to travel they will need:
- First and last name.
- Date of birth.
- Either Social Security number, Medicaid identification number, or health care member identification number.
For more information on how to use WIR or access it in another language please visit the Wisconsin DHS Immunization Program Web page.
Frequently asked questions about using WIR
I had vaccines that are missing from WIR. How do I correct it? Travelers should provide proof that they had the vaccine to their health care provider's office or local health department, and they can enter the traveler’s vaccine information for them.
If I got a vaccine in another state, will it be in WIR? Maybe. WIR shares information with Minnesota and Michigan. If travelers had a Wisconsin address when they got the vaccine in one of those states, WIR may have a record of the vaccine.
How do I locate my vaccination records if they are not in WIR? Unfortunately, there is no national organization that maintains vaccination records. The records that exist are the ones travelers or their parents were given when the vaccines were administered and the ones in the medical record of the doctor or clinic where the vaccines were given.
If travelers need official copies of vaccination records, or if they need to update their personal records, there are several places they can:
- Ask parents or other caregivers if they have records of their childhood immunizations.
- Look through baby books or other saved documents from their childhood.
- Check with their high school or college health services for dates of any immunizations. Keep in mind that generally records are kept only for 1–2 years after students leave the system.
- Check with previous employers (including the military) that may have required immunizations.
- Check with their health care provider or public health clinic. Keep in mind that vaccination records are maintained at health care provider's office for a limited number of years.
What do I do if I can’t find my records? If travelers can’t find their personal records or records from their health care provider, they may need to get some of the vaccines again. While this is not ideal, it is safe to repeat vaccines. Health care providers can also sometimes do blood tests to see if they are immune to certain vaccine-preventable diseases.
CDC Travel Health Notices for International Travelers
Level 4 – Avoid All Travel
None at this time.
Level 3 – Reconsider Non-Essential Travel
None at this time.
Level 2 – Practice Enhanced Precautions
Mpox in the Democratic Republic of the Congo (DRC)
The CDC has updated the level 2 travel notice for an Mpox outbreak in 25 of 26 provinces in the DRC. Mpox is caused by the monkeypox virus and is endemic throughout Central and West Africa near forests. Person-to-person transmission has occurred during this outbreak including through sexual contact, household contact, and within health care settings. Vaccination against mpox is recommended for people with certain risk factors. Additional prevention strategies for travelers can be found on the CDC Travelers’ Health Mpox web page. Travelers should seek care immediately if they develop a new, unexplained skin rash, with or without fever and chills and should avoid contact with others.
Chikungunya in Maldives
The CDC has updated the level 2 travel health notice for an outbreak in Maldives. Chikungunya disease is caused by the chikungunya virus and is spread to humans through mosquito bites. Anyone traveling to Maldives should take steps to prevent mosquito bites. Pregnant travelers should reconsider travel to Maldives. Chikungunya virus can infect the baby before or during delivery and can result in severe illness to the newborn. Travelers with symptoms of fever, joint pain, headache, muscle pain, joint swelling, or rash should seek medical care during or after travel.
The CDC issued an updated level 2 notice for global polio. Polio is a crippling and potentially deadly disease that affects the nervous system. Polio has been eliminated from most of the world, but some international destinations have circulating poliovirus. Before any international travel, adults and children should make sure they are up to date on polio vaccines. In countries where there is an increased risk of exposure to poliovirus, travelers may be required by the government of that country to show proof of polio vaccination when departing that country.
Level 1 – Practice Usual Precautions
Disease Spotlight: Legionnaires’ Disease
Legionnaires’ disease is a severe type of pneumonia that is caused when Legionella bacteria are inhaled. While Legionella is found in freshwater environments (such as lakes and rivers) worldwide, Legionella is most likely to grow and amplify in building water distribution systems and water-aerosolizing devices. Patients diagnosed with Legionnaires’ disease often report traveling during the two weeks before their illness. Legionnaires’ disease has been increasingly reported in Wisconsin, with over 200 cases reported to public health per year each year since 2018.
Who is at risk?
Not all individuals who are exposed to Legionella bacteria will have symptoms of Legionnaires’ disease. People with compromised immune systems or underlying medical conditions, such as chronic obstructive pulmonary disease (COPD), obstructive sleep apnea, or cardiovascular disease are more likely to become ill. People over 50 years of age and people who currently smoke are also at increased risk.
What are the symptoms?
Common signs and symptoms of Legionnaires’ disease include:
- Cough
- Fever
- Shortness of breath
- Fatigue
- Headache
- Diagnostic imaging findings suggesting pneumonia, consolidation, or pulmonary infiltrates
Additional symptoms include:
- Sudden increase in confusion or change in mental status
- Chest pain
- Gastrointestinal symptoms, such as diarrhea
How is it spread?
Legionella bacteria grow and amplify in water distribution systems (which can include buildings, mobile homes, or recreational vehicles) and water-using devices (for example, hot tubs, decorative fountains, or humidifiers) that are not adequately maintained. Disease can occur when people inhale aerosols from a water source containing Legionella (examples include showers, sinks, or misters). Cooling towers, which are sometimes used for cooling large buildings, can be a source of Legionella spread. Home and car air conditioners are not thought of as a source of Legionella spread since these devices do not use water. Legionnaires’ disease is not spread from person to person. This CDC infographic has more information on factors for Legionella growth in the environment.
Diagnostics
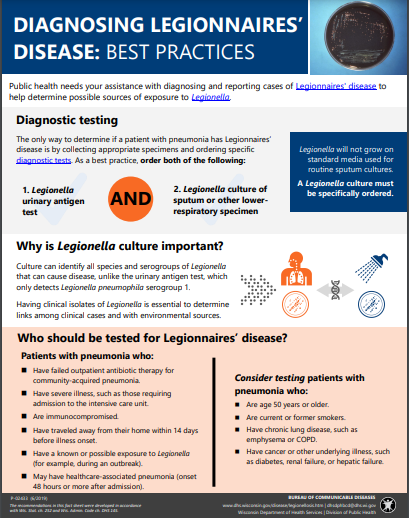
For patients diagnosed with community-acquired pneumonia, Legionnaires’ disease is most frequently diagnosed with a urine antigen test. Urine antigen tests are able to detect infections caused by Legionella pneumophila serogroup 1, which accounts for about 80% of Legionnaires’ disease cases.
Culture or PCR of lower respiratory specimens (such as sputum or bronchoalveolar lavage) detects Legionnaires’ disease caused by other species and serogroups of Legionella. Since Legionella does not grow on routine respiratory culture media, Legionella culture must be specifically ordered. Isolates from Legionella culture allow public health to directly compare patients to environmental isolates obtained from outbreak investigations.
See the Diagnosing Legionnaires’ Disease: Best Practices fact sheet for additional information on testing.
Treatment
Most patients with Legionnaires’ disease who get sick need care in a hospital but make a full recovery. Patients who are immunocompromised are at greater risk of severe illness. Legionnaires’ disease is treatable with antibiotics, specifically respiratory fluoroquinolones (such as levofloxacin) or macrolides (such as azithromycin). Note that Beta-lactam antibiotics that are often used as first line treatment to treat community-acquired pneumonia are generally not effective for treating Legionnaires’ disease.
Travel recommendations
Consider testing for Legionnaires’ disease for patients that present with community-acquired pneumonia and traveled within 14 days before becoming ill.
|
|

