
This update is being sent to members of the Wisconsin Travel Health Network.
Global Health Update
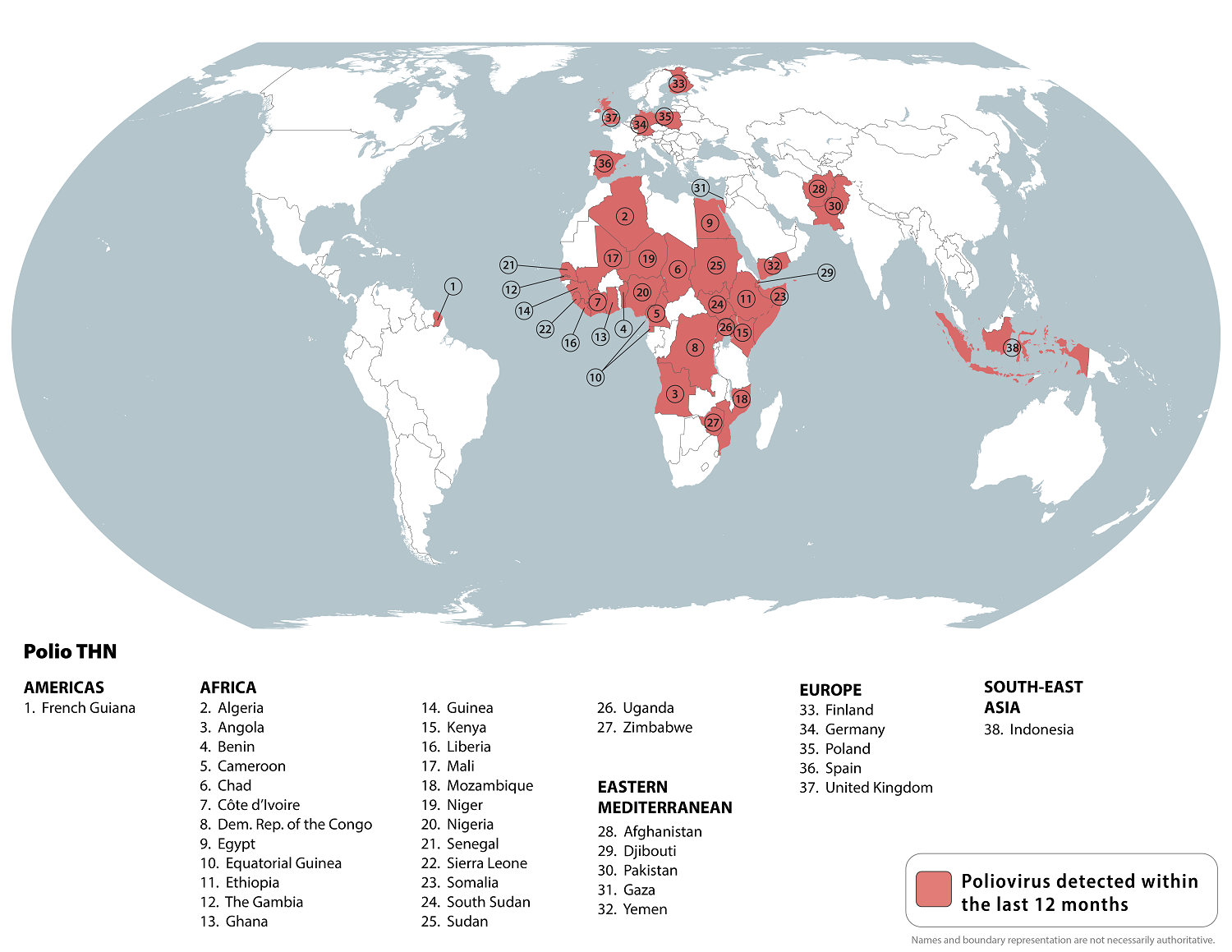
Global polio
The Centers for Disease Control and Prevention (CDC) issued a Level 2 Alert for global polio. Polio has been eliminated from most of the world, but some international destinations have circulating poliovirus. Before any international travel, adults and children should make sure they are up to date on polio vaccines. Before travel to any destination with poliovirus detected within the last 12 months, adults may additionally receive a single, one-time booster dose of inactivated polio vaccine (IPV). In countries where there is an increased risk of exposure to poliovirus, travelers may be required by the government of that country to show proof of polio vaccination when departing that country.
Locally acquired malaria cases identified in the U.S.
On June 26, the CDC issued a Health Alert Network (HAN) Health Advisory to notify health care providers and public health authorities of identification of five locally acquired malaria cases in Florida and Texas within the previous two months. The CDC also raised concern for a potential rise in imported malaria cases associated with increased international travel this summer. Finally, the memo discussed the need to plan for rapid access to IV artesunate, the first-line treatment for severe malaria in the United States.
Review the bulletin sent on June 30 for background information, information on malaria in Wisconsin, recommendations for clinicians and other health care entities in Wisconsin, and additional resources.
If you were unable to attend live, review the recording of the July 20 CDC COCA Call: Review of Malaria Diagnosis and Treatment in the United States. This call covers how to prevent, diagnose, and treat malaria; how the biology of the pathogen contributes to clinical management of the disease; and how CDC and state and local health departments are responding to the locally acquired mosquito-borne malaria cases in the United States.
Travel-associated disease case finding
DHS routinely receives alerts from other state health departments regarding clusters or outbreaks of disease that may cause illness in out-of-town visitors or guests of a particular facility, venue, or event. The local and state health departments investigating the cluster recognize that although exposure to the pathogen may have occurred in their jurisdiction, some travelers may manifest symptoms of illness and seek medical evaluation after leaving the area. Examples of these alerts include:
- Call for cases: Enteric Illness Associated with Drinking Untreated Water in Vacation Destination—Island Park, Idaho
Eastern Idaho Public Health is requesting to be notified if public health jurisdictions outside of Idaho identify any enteric illness in a person who visited Island Park and drank un-boiled tap water during the possible exposure period. Please report cases.
- Call for Cases: Pertussis Associated with Spiritual Gathering in Ohio—June 9, 2023
The Ohio Department of Health (ODH) and the Darke County General Health District are investigating an outbreak of pertussis among attendees of a large spiritual gathering held in West Milton, Ohio between May 21–28, 2023. Please report potentially associated cases.
- Call for Cases: Legionnaires’ Disease Cases Associated with a Hotel in Atlantic City, New Jersey—June 22, 2023
New Jersey public health officials are investigating several cases of Legionnaires’ disease associated with a hotel and casino in Atlantic City, New Jersey. Health departments are asked to notify the New Jersey Department of Health of similar cases.
These “call for cases” and alerts are coordinated by the CDC and highlight the importance of obtaining a thorough travel and exposure history for patients presenting with symptoms of an infectious disease. Those extra details can raise the clinical suspicion for non-routine diseases, lead to earlier diagnosis and treatment of travel-associated diseases, and assist health departments with identifying cases associated with a particular event or location in Wisconsin or elsewhere.
Disease Spotlight: Typhoid Fever and Paratyphoid Fever
Typhoid fever and paratyphoid fever are potentially life-threatening illnesses caused by the bacteria Salmonella Typhi and Salmonella Paratyphi, respectively. Typhoid fever and paratyphoid fever are rarely diagnosed in Wisconsin residents and when they are, people most often have traveled to regions with a high risk of both illnesses, including parts of Asia (especially South Asia), Latin America, and Africa. Worldwide, it is estimated that there are 11–21 million typhoid fever infections and about 5 million paratyphoid fever infections each year.
Who is at risk?
Any person can get typhoid or paratyphoid fever but people who travel to countries where the diseases are more common are at increased risk. It is important to take preventative measures when traveling to these countries such as getting vaccinated (for typhoid fever) at least one week prior to travel, drinking bottled water, and avoiding uncooked foods and drinks with ice.
What are the symptoms?
Symptoms of both typhoid fever and paratyphoid fever usually start between six and 30 days after a person is exposed but may take up to three months for typhoid fever. People who develop a high fever and feel very ill after having contact with someone with typhoid fever or after traveling to countries where typhoid fever and paratyphoid are common should seek health care immediately.
Common signs and symptoms:
- High, sustained fever (a fever that does not come and go)
- Fatigue
- Loss of appetite
- Headache
- Diarrhea or constipation
- Abdominal pain
Other signs and symptoms:
- Dry cough
- Sore throat
- Myalgias (muscle pain)
- Rash
How is it spread?
Both typhoid fever and paratyphoid fever are spread through sewage contamination of food or water and through contact with an infected person. People who have recovered can also still carry the bacteria and infect other people. The bacteria that cause typhoid fever and paratyphoid fever are not spread by animals.
What are the diagnostic challenges?
Both diseases are diagnosed by isolating Salmonella Typhi or Salmonella Paratyphi from either the blood, stool, or bone marrow of infected people. Multiple blood cultures may be needed to make a diagnosis as single cultures are positive only in about half of cases. Stool cultures are less sensitive than blood cultures and may not be positive in the first week of a person’s illness. Bone marrow cultures, while invasive, have greater sensitivity than either blood or stool cultures and are less affected by antibiotic use. Because of the time it can take to get a positive culture result, often the initial diagnosis must be made clinically based on symptoms and travel history.
While several commercial serologic tests are available, these have both poor sensitivity and specificity and should not be used as the sole means of diagnosis.
Is there treatment for typhoid fever?
There are two typhoid fever vaccines approved for use in the United States and vaccination prior to travel to areas where typhoid fever is common may reduce the risk of becoming infected.
Typhoid fever and paratyphoid fever are treated with antibiotics. Because Salmonella Typhi is increasingly resistant to many antibiotics, empiric treatment decisions in cases where typhoid fever is suspected should be informed by a patient’s travel history pending culture results. Further treatment should be guided by antibiotic susceptibility test results if the bacteria is successfully isolated from a patient’s blood, stool, or bone marrow.
If you or a family member has recently traveled to an area with typhoid fever and paratyphoid fever have symptoms, contact a health care provider.
|


{kind=link}