|
COVID-19 Health Alert # 23:
Options for Reducing the Duration of Quarantine for Individuals Exposed to COVID-19
Bureau of Communicable Diseases, December 4, 2020
Summary
- Quarantine, defined as the strict physical separation of individuals who have been exposed to a communicable disease, is an essential strategy for preventing the spread of COVID-19. Ideally, quarantine should be continued for the full incubation period (i.e., the period during which an exposed person is at risk for becoming infectious), which for the SARS-CoV-2 virus is 14 days.
-
In accordance with recently revised CDC guidelines, DHS supports shortening the standard quarantine period from 14 days to 10 days for people who remain asymptomatic, provided that daily symptom monitoring continues for the full 14 day period. This change is based on modeling data suggesting that the residual risk of transmission is very low after 10 days, and the expectation that a less burdensome requirement may improve community compliance with quarantine and contact tracing.
- The duration of quarantine may be further shortened to 7 days using a test-based strategy. Individuals may be released from quarantine after 7 days if an FDA authorized diagnostic test (PCR or antigen) is collected within 48 hours of the proposed end of quarantine (i.e. on day 6 or 7 of quarantine), the result is negative, and that symptom monitoring continues for the full 14 day period. This is a change from previous CDC and DHS guidance that quarantine should continue for 14 days regardless of any test results.
-
DHS has previously recommended (HAN #18 and HAN #22) that quarantined healthcare personnel may be asked to work in patient care settings during critical staffing shortages, using a strategy of serial testing during the 14 day quarantine period. Because of the non-zero risk of developing infection between days 7-14 following exposure, and the potential risk this creates for patients, DHS continues to recommend strict symptom monitoring and serial testing for 14 days while HCPs are on duty, even if they have met the community standard for shortened quarantine.
- Shortened quarantine duration may not be appropriate in all settings. High-risk, congregate settings such as long-term care facilities, shelters, jails and prisons must determine on a case by case basis whether potential benefits of shortened quarantine outweigh the risks of post-quarantine transmission.
Dear Colleagues,
This week, the U.S. Centers for Disease Control and Prevention released an updated guidance document entitled Options to Reduce Quarantine for Contacts of Persons with SARS-CoV-2 Infection Using Symptom Monitoring and Diagnostic Testing. Wisconsin healthcare providers and public health partners are encouraged to review the new CDC guidance closely, as the document describes several important modifications to the existing practice around quarantine for persons exposed to the SARS-CoV-2 virus.
Wisconsin DHS has reviewed the modified guidance and its scientific rationale, and is in agreement with CDC that the two options for reducing the duration of quarantine are acceptable and may have numerous public health benefits if implemented appropriately. DHS acknowledges that these alternative strategies represent a substantial change from previous guidance, and that partner organizations and community members may have questions about this new guidance. For these reasons, DHS recommends that local and tribal health departments implement these changes no earlier than Monday, December 7, 2020. The two alternative strategies for discontinuation of quarantine are listed below:
- Quarantine can end after Day 10 without testing, if no symptoms have been reported during daily monitoring.
- Quarantine can end after Day 7 if the result of a diagnostic COVID-19 test is negative and if no symptoms were reported during daily monitoring. The test specimen may be collected and tested within 48 hours before the time of planned quarantine discontinuation but quarantine cannot be discontinued earlier than after Day 7. A pending test result on day 7 is not sufficient to end quarantine early.
For these two alternative strategies to be acceptable, the following conditions must be met:
- Daily symptom monitoring must continue for all individuals in quarantine through Day 14.
- No clinical evidence of COVID-19 has been elicited by daily symptom monitoring during the entire period prior to the end of quarantine.
- Persons must be advised that if symptoms develop at any time, they should immediately self-isolate and contact the local public health authority or their healthcare provider to report this change in clinical status.
- Persons must be counseled regarding the need to adhere strictly to all recommended non-pharmaceutical interventions, (i.e., consistent mask use, social distancing, and avoiding gatherings) for the full 14 days after exposure.
Highlighted below are additional considerations that DHS believes are important to communicate with partners.
Quarantine for 14 full days after the time of exposure remains the safest strategy for preventing asymptomatic transmission of SARS-CoV-2. The recommendation for a 14-day quarantine is based on estimates of the upper bounds of the COVID-19 incubation period, that is, the period of time during which nearly all individuals who develop infection will become infectious. The rationale behind shortened quarantine is NOT because our understanding of the incubation period of the virus has changed. Rather, the alternative strategies are deemed acceptable because the residual risk of transmission after the shortened duration is small, and this risk may be outweighed by the potential benefits of a quarantine requirement that places less burden on individuals, families and communities. Table 1 displays the results of modeling studies conducted by CDC that aim to estimate the residual risk after shortened quarantine, provided that quarantined individuals continue daily symptom monitoring for 14 days and immediately isolate if they become symptomatic.
Table 1. Estimated residual post-quarantine transmission risk with and without a negative diagnostic test result. (Source: CDC)
|
Planned day after which quarantine is completed and can be discontinued
|
Residual post-quarantine transmission risk (%) with and without diagnostic testing of a specimen within 48 hours before time of planned discontinuation of quarantine
|
|
No testing
|
RT-PCR testing
|
Antigen testing
|
|
Median
|
Range
|
Median
|
Range
|
Median
|
Range
|
|
7
|
10.7
|
10.3-22.1
|
4.0
|
2.3-8.6
|
5.5
|
3.1-11.9
|
|
10
|
1.4
|
0.1-10.6
|
0.3
|
0.0-2.4
|
1.1
|
0.1-9.5
|
|
14
|
0.1
|
0.0-3.0
|
0.0
|
0.0-1.2
|
0.1
|
0.0-2.9
|
Testing for the purpose of reducing quarantine duration should be done only when diagnostic testing resources are sufficient and available. The CDC guidance is intended to apply to settings where implementing testing for early discontinuation of quarantine does not divert testing resources away from individuals who require diagnostic testing. On a state-wide level, DHS believes there are sufficient testing resources to make implementation of the test based strategy a reasonable community standard. In fact, DHS has and continues to recommend that all individuals who are in quarantine because of close contact to a case should be tested during their quarantine period, as a key strategy for identifying people with asymptomatic infection. As testing resources are subject to change, however, local jurisdictions and health care organizations may determine whether emerging resource limitations make the test-based strategy infeasible.
Point of care antigen tests are acceptable to use for the purpose of reducing duration of quarantine, but molecular (e.g. PCR) tests are preferable. Antigen tests, when used for testing asymptomatic patients, are known to have lower sensitivity that molecular tests. The modeling data shown in Table 1 was conducted with an assumption that antigen tests have a 70% diagnostic sensitivity in comparison to PCR. The estimated residual post-quarantine transmission risk after 7 days is therefore slightly higher (5.5% vs. 4.0%) when antigen tests are used. This higher risk must be balanced against the benefits of antigen tests, including their more rapid turnaround time and lower cost.
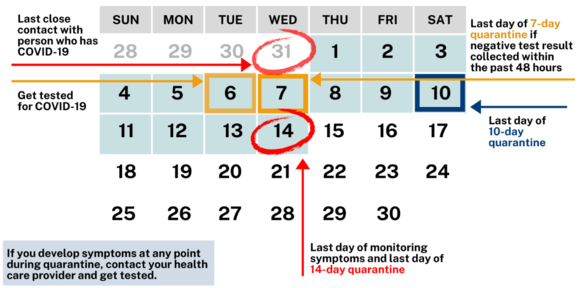
The timing of test collection must be no earlier than 48 hours before the anticipated end of quarantine. As shown in the figure below, day 1 of quarantine is the day after the last known exposure. Individuals may return to work or other activities involving contact with others the next day following the last quarantine day (i.e. on day 15 if using a 14 day quarantine). The last day of quarantine for each of the three options is indicated in the figure. To meet the 48 hour requirement, specimen collection for the 7-day quarantine option could occur on day 6 or 7, as shown below.
Figure 1. Quarantine guidance for close contacts of COVID-19 cases
 High-risk, congregate settings such as long-term care facilities, shelters, jails and prisons must determine on a case by case basis whether potential benefits of shortened quarantine outweigh the risks of post-quarantine transmission. As noted above, quarantine for a full 14 days remains the safest way to prevent transmission from asymptomatically infected people. A residual post-quarantine transmission risk of 5% means that one out of twenty exposed individuals who end quarantine after 7 days with a negative test may develop infection and place others in their facility at risk for COVID-19. This risk may be unacceptably high in some environments where vulnerable individuals reside, or where crowded conditions increase the likelihood that a single case could lead to a large outbreak.
We at DHS thank you for your collaboration and support in consideration of these changes.
Sincerely,
Ryan Westergaard, MD, PhD, MPH Chief Medical Officer and State Epidemiologist for Communicable Diseases Wisconsin Department of Health Services
About the COVID-19 Health Alert Network
The content of this message is intended for public health and health care personnel and response partners who have a need to know the information to perform their duties. The HAN will be the primary method for sharing time-sensitive public health information with clinical partners during the COVID-19 response. Health care providers and other officials can subscribe and unsubscribe using their preferred email address at the DHS COVID-19 website.
I received your message
|
