|
Childhood Vaccine Program provider agreement renewal is upon us! Renewals are organized by county so please check out the Renewal Schedule. We have resources available to help you with this process:
If you haven't done so yet, ensure your clinic is ready to renew by completing the following:
- Gather practice profile data for the calendar year 1/1/24 - 12/31/24
- Ensure all thermometer calibrations are up to date
-
New annual training requirements for primary and back-up vaccine coordinators completed within the current calendar year (2025)
Please join us Thursday, March 27, 2025 for our next CVP Training Series. This month we will be covering program billing guidelines, eligibility screening and documentation.
Topic: Billing and Eligibility Screening
Date: March 27, 2025
Time: 12 noon
Primary Audience: Billing Coordinators, Providers and Vaccine Coordinators for the Childhood Vaccine Program
Register Here
While the onset and duration of RSV season may vary throughout the United States, nirsevimab is typically administered October through the end of March in most of the continental US.
Healthcare providers should stop administering nirsevimab by March 31. Nirsevimab will no longer be available for ordering through the Childhood Vaccine Program after March 14, 2025.
Remaining inventory of nirsevimab is viable until its expiration date. Product should continue to be safely stored refrigerated between 36°F to 46°F (2°C to 8°C) and can be used when administration resumes next season. More information can be found here: Frequently Asked Questions About RSV Immunization with Monoclonal Antibody for Children 19 Months and Younger | CDC
Please don't hesitate to contact us at WAChildhoodVaccines@doh.wa.gov for any questions or for assistance managing your nirsevimab inventory.
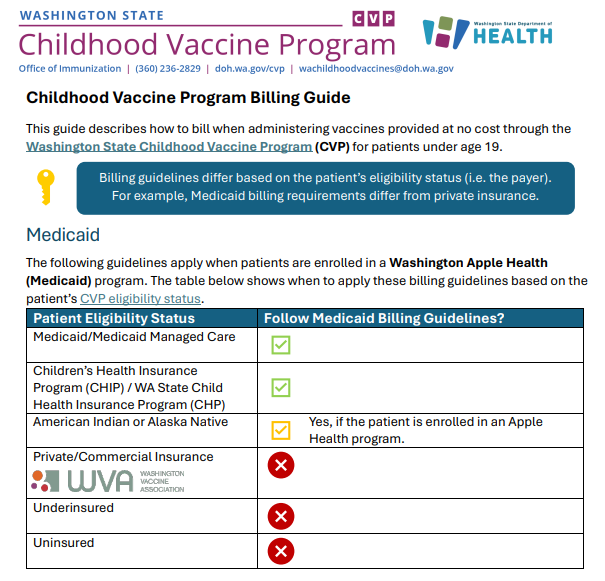
We have a new billing guide available that provides an overview of Childhood Vaccine Program billing requirements, including how to bill Medicaid, self-pay patients, and the required private/commercial insurance dosage-based assessment (DBA). We encourage sharing this new resource with your billing staff, so they have the resources needed to bill according to program requirements.
We have two new documents that will help in your efforts to reduce vaccine waste:
The Reducing Vaccine Waste Toolkit covers best practices and options for managing your clinic's inventory of short dated vaccines. There are multiple tools available in the IIS to help manage your inventory including the Vaccine Lots to Expire report.
The Vaccine Lots to Expire Report Guide covers how to run the Vaccine Lots to Expire report, which can be utilized to manage vaccine inventory and find your shortest-date vaccine.
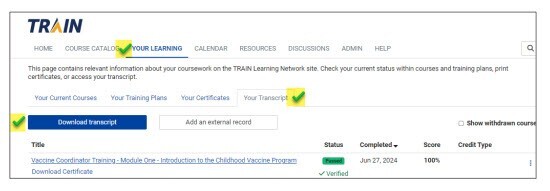
As a reminder, when you have completed your annual Vaccine Coordinator Training, please be sure to print a training transcript and put it in your Childhood Vaccine Program binder (in lieu of individual module certificates). The training transcript is the documentation that will be checked during your site visit.
Printing a Training Transcript in TRAIN.org:
o Select the YOUR LEARNING tab at the top of the page
o Click on Your Transcript
o Your completed courses will be listed
o Click on the Download Transcript button
o Please print the transcript and put it in your Childhood Vaccine Program binder
Beginning March 10, McKesson will be using new electronic TagAlert temperature monitors for refrigerated vaccine shipments.
These monitors are similar to the ones that are currently being used in the frozen Moderna COVID shipments, and they monitor both warm and cold excursions during the shipment. McKesson will continue to use a qualified cooler and pack out, in addition to these new monitors.
A guide that includes information about the new temperature monitor will be included in refrigerated vaccine shipments.
Washington State Department of Health’s Power of Providers (POP) initiative invites you to participate in an upcoming webinar series focused on behavioral health support for health care professionals. The series will begin with Health for Health Care Professionals: Taking Care of Yourself as You Care for Others and features Washington’s prominent disaster psychologist, Dr. Kira Mauseth. This is part one of a three-part series. Please visit POP's webinar page for more information on the rest of the series.
Date: Wednesday, March 19th, 2025
Time: 12 noon
Register here
The learning objectives for this webinar are to:
- Identify experiences that contribute to burnout vs restoration.
- Develop a personal plan for healthy engagement.
- Establish healthy boundaries around work and “off” time.
The webinar will be recorded and there will be live ASL interpretation. We are offering free continuing education for nurses, medical assistants, pharmacists and pharmacy technicians.
CDC issued a measles Health Alert Network (HAN) advisory to notify clinicians and potential travelers about a measles outbreak in Texas and New Mexico, and offer guidance for prevention and monitoring.
Recommendations for Healthcare Professionals
Ensure all patients without other evidence of immunity, especially those planning international travel, are up to date on MMR vaccine per routine ACIP recommendations:
- Children are recommended to receive 2 doses of MMR. The first dose is given at 12–15 months of age and the second is given at 4–6 years of age before school entry.
- Infants 6 months of age or older can receive MMR prior to international travel or in outbreak settings (see below). MMR is not licensed for children <6 months of age.
- Adults not at high risk of exposure are recommended to have at least 1 documented dose of MMR in their lifetime, or other evidence of immunity (e.g., positive measles immunoglobulin G (IgG)). Adults at high exposure risk, including students at post-secondary institutions, healthcare workers, and international travelers, should have two documented doses.
Ensure patients who reside in areas with an ongoing measles outbreak follow state and local guidance. Texas Department of State Health Services (DSHS) issued specific recommendations for the affected counties in Texas.
Ensure all U.S. residents older than age 6 months without evidence of immunity who are traveling internationally receive MMR vaccine prior to departure:
- Infants 6 through 11 months of age should receive one dose of MMR vaccine before departure. Infants who receive a dose of MMR vaccine before their first birthday should receive 2 more doses of MMR vaccine; the first of which should be administered when the child is 12 through 15 months of age and the second at least 28 days later (generally at age 4-6 years of age but can be administered sooner if indicated).
- Children 12 months of age or older should receive two doses of MMR vaccine, separated by at least 28 days.
- Teenagers and adults without evidence of measles immunity should receive two doses of MMR vaccine separated by at least 28 days.
Be aware that some patients may develop a mild rash reaction in the 3 weeks following MMR vaccination. This does not typically require testing or public health intervention since a person with a rash due to a vaccine reaction is not infectious. If a symptomatic person who has been recently vaccinated also has a known or suspected measles exposure, consultation and additional testing may be required from the local or state health department to evaluate for acute measles.
Additional Resources:
National and WA Measles Cases
Measles outbreaks are becoming an increasing concern in 2025. The CDC reports that as of March 6, 2025, there have been 222 measles cases reported in 12 states. Currently, there are ongoing outbreaks occurring in Texas and New Mexico. As of March 7, 2025, the Texas Department of State Health Services reported an outbreak in the South Plains region, with 198 cases identified since late January. Twenty-three of the patients have been hospitalized. Vaccination status is unknown in 113 of the cases, 80 cases are not vaccinated, and 5 cases report being vaccinated with at least one dose. Investigations into the cases who are currently classified as vaccinated are ongoing. There has been one fatality in a school-aged child who lived in the outbreak area. The child was not vaccinated and had no known underlying conditions. As of March 7, 2025, New Mexico reported 10 cases. There has been one fatality reported in an unvaccinated adult who tested positive for measles.
As of March 7, 2025, Washington has had one confirmed case of measles this year. This case may have been exposed during recent travel abroad. Outbreaks ranging in size from seven to 33 cases occurred in Washington in 2001, 2004, 2008, and 2014. In 2015, one outbreak occurred with six cases, one of which was fatal. In 2019, there were two large outbreaks of measles in addition to four non-outbreak cases, totaling 90 cases. Since then, Washington has experienced sporadic cases and small outbreaks due to unvaccinated persons being exposed to measles during travel to areas where measles is circulating. There were six confirmed cases of measles in Washington state in 2024. All six cases either had or were linked to international travel. Most cases have been among people 12 months of age or older who had not received measles, mumps, and rubella (MMR) vaccine.
People infected with measles can spread the virus by coughing or sneezing. The virus may remain in the air for 2 hours after an infected person has left. Symptoms of measles include fever, cough, runny nose, and red, watery eyes. A full-body rash typically develops on the head or face and spreads down the body. People with measles are contagious for up to four days before their rash even begins. People who have been exposed to measles may become ill between 7 and 21 days after the exposure. The only treatment for a measles infection once it occurs is over the counter (OTC) products for symptom relief. Unvaccinated infants, young children, pregnant persons, and those who are immunocompromised are at highest risk of severe measles complications, which can include pneumonia, encephalitis, brain damage, pregnancy complications and even death. The MMR vaccine is the strongest protection against measles. Two doses of measles-containing vaccine are approximately 97% effective at preventing measles. The spread of measles can be stopped in communities by maintaining 95% or higher measles vaccination coverage.
For Healthcare Providers:
DOH recommends healthcare providers follow 5 steps when dealing with potential measles cases:
-
Isolate: Keep patients with a rash and fever away from shared spaces. Keep the patient in an airborne infection isolation room or a private room with a closed door.
-
Notify: Immediately notify your local health jurisdiction (LHJ) about suspected cases to ensure testing and investigation.
-
Test: Work with your LHJ to get approval to test for measles through the Washington State Public Health Laboratories.
-
Manage: Provide appropriate measles post-exposure prophylaxis (PEP) to close contacts without evidence of immunity in coordination with your LHJ.
-
Vaccinate: Make sure all your patients are up to date on MMR vaccine, especially before international travel.
MMR Vaccine Recommendations for Younger Children and Adults
CDC currently recommends a measles, mumps, and rubella (MMR) vaccine for children 6 months or older if they are travelling internationally or in a community outbreak. There is no current recommendation to give MMR vaccine for travel in the US or if there’s concern about the possibility of being exposed. The Washington Childhood Vaccine Program follows CDC and ACIP (Advisory Committee on Immunization Practices) recommendations and we will notify providers if the recommendations change.
Adults should be up to date on MMR vaccinations with either 1 or 2 doses, depending on risk factors, unless they have evidence of immunity:
- Written documentation of MMR vaccine
- Lab evidence of immunity or lab confirmation of disease
- Birth before 1957
Live-attenuated measles vaccine became available in the U.S. in 1963. An ineffective, inactivated measles vaccine was also available in the U.S. in 1963–1967. Adults who received a dose of measles vaccine in 1963–1967 and are unsure which type of vaccine it was, or are sure it was inactivated measles vaccine, should be revaccinated with one or two doses of MMR vaccine. More information about the number of MMR vaccines recommended for adults can be found at Ask The Experts About Vaccines: MMR (Measles, Mumps, and Rubella) | Immunize.org.
Additional Resources:
Due to unforeseen circumstances, the Pink Book Training has been cancelled this year. WithinReach hopes to offer this essential training course in future years when the logistics can come together. In the meantime, WithinReach is partnering with Washington Department of Health, the American Indian Health Association, and local coalitions to plan an alternate virtual learning series for health professionals “Building Immunity, Strengthening Communities” on June 2 – 5 from 12 – 2 PM. Join us for clinical best practices and strategies for vaccine administration, increasing vaccine confidence, and more. CEUs will be available, agenda and specific presentation topics coming soon.
For questions about the immunization schedule, the Immunization Information System forecast, or any other immunization clinical questions, please send an email to ImmuneNurses@doh.wa.gov. Check out the Immunization Training web page for more resources and training opportunities.
When renewing your facility's provider agreement in the IIS, remember to enter your thermometer's make and model in the field labeled "serial number". We do not require the serial number. This information can typically be found on your certificate of calibration.

|