
HERC Spotlight: February 2026
Veterans Health Administration sent this bulletin at 02/04/2026 11:23 AM EST
Health Economics Spotlight
|
||
In This Issue |
SpotlightMethods for Economic Evaluations of VA ProgramsThere are several ways to evaluate the cost of VA programs. The methods you use will depend on the question you’re trying to answer and the available data. Here, we review three different methods with examples from recent studies. Causal inference or quasi-experimental methods such as difference-in-differences (DID) can be used when randomized clinical trials are not feasible. |
|||
|
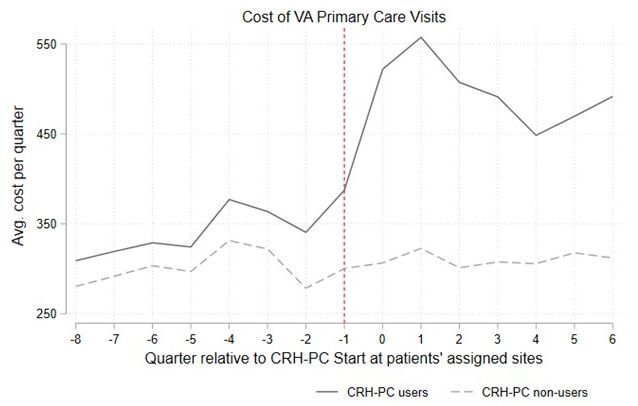
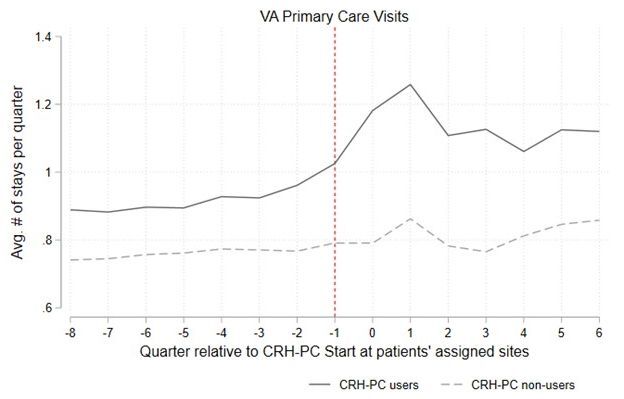
At VA, economic evaluations analyses can be conducted using CDW data, making this a pragmatic option in many projects. These methods can study health outcomes and health benefits alongside costs. Learn more about DID and other quasi-experimental methods in the seminar, “Options for Evaluating VA Programs.” Other HERC cybserminars also highlight common quasi-experimental methods. DID in practice: Impact of VA’s Clinical Resource Hub primary care telehealth program. |
Unadjusted descriptive trends in mean cost and utilization for CRH-PC users and non-users |
||
|
Conduct a traditional cost-effectiveness analysis (CEA) to determine if the value of an intervention justifies its cost. CEAs, which are often conducted alongside a clinical trial, are considered the gold standard for measuring value. However, CEAs have several downsides: models are difficult to create, and they can be expensive and time-consuming. Studies often need access to clinical trial data rather than relying solely on CDW data. Before undertaking a CEA, researchers should decide on the perspective (e.g., societal or payer) and time horizon (long term or short term) as these may affect which costs should be included. Learn more about conducting a CEA during the February HERC seminars. CEA in practice: Cost effectiveness of psychotherapy delivery methods for PTSD Results indicate that all delivery formats can be beneficial and cost-effective; therefore, it is recommended clinicians engage in a shared decision-making process to determine the preferred and optimal delivery format for each patient. Microcosting allows for examining the cost of a program. Sometimes decision makers just want better information on what it costs to implement a new program. Microcosting is a method for measuring costs in these situations. In microcosting, a cost is derived for each element of an intervention: staff time, supplies, other IT costs, etc. Given the level of detail needed, the study team may need to collect data as existing sources of data may be inefficient. Microcosting in practice: Improving access to buprenorphine and naltrexone for persons with opioid use disorder Citations Gujral K, Scott JY, Dismuke-Greer, et al. Impact of VA’s Clinical Resource Hub Primary Care Telehealth Program on Health Care Use and Costs. Medical Care. 2025 September 22. Moring JC, Dismuke-Greer CE, Resick PA, et al. Cost-effectiveness of evidence-based psychotherapies for PTSD: An examination of different treatment delivery modalities. Psychol Serv. 2026 Jan 26. Wagner TH. Rethinking How We Measure Costs in Implementation Research. J Gen Intern Med. 2020 Nov;35(Suppl 2):870-874. |
|||
February SeminarsCost-Effectiveness Analysis - From Methods to PracticeCost-effectiveness analysis is a tool used to aid decisions about which medical care should be offered. It is a method of comparing the cost and effectiveness of two or more alternatives. Such comparisons are useful when one of the alternatives being considered is standard care, as this allows the decision maker to consider whether an innovation is better than the status quo. The goal of cost-effectiveness analysis to determine if the value of an intervention justifies its cost. This February, we are featuring two seminars on cost-effectiveness analysis (CEA). On February 11, Jeremy Goldhaber-Fiebert (Stanford University) will discuss methods for conducting a CEA. Then, on February 25, Marika Cusick (Johns Hopkins Bloomberg School of Public Health) will walk through an example of a CEA. All seminars are open to VA participants only until further notice. Advanced Decision Science MethodsHERC Cost-Effectiveness Analysis Seminar Wednesday, February 11 at 1pm ET |
|||
Register |
|||
|
|
|||
|
This seminar will review topics such as microsimulation, probabilistic sensitivity analysis, model calibration and validation, and introduce value of information. Intended audience: Researchers who would like an introduction to methods of cost-effectiveness analysis as applied to health services and medicine. |
|||
Cost-Effectiveness of Dapagliflozin in Non-Diabetic Chronic Kidney Disease: A Cost-Effectiveness Analysis Case StudyHERC Cost-Effectiveness Analysis Seminar Wednesday, February 25 at 1pm ET |
|||
Register |
|||
|
|
|||
|
In this cyberseminar, Dr. Cusick will present a published cost-effectiveness analysis on the inclusion of dapagliflozin in the standard of care for non-diabetic chronic kidney disease (CKD). This applied decision analysis builds on evidence from the 2020 DAPA-CKD clinical trial, which demonstrated dapagliflozin’s efficacy in CKD patients with and without diabetes. This webinar uses this study as an example of cost-effectiveness analyses applied to health and medicine. Intended audience: Researchers seeking an introduction to applied cost-effectiveness analyses in medicine, public health, or health services. |
|||
ResourcesHERC Datasets Updated for FY25HERC's Inpatient Average Cost data and VHA Labor Cost dataset (VA intranet only) are updated with FY25 data. HERC’s average cost data includes encounter-level cost estimates of VA care. The estimates represent the national average cost of a hospital stay given its Diagnosis Related Group (DRG), overall length of stay, and days in intensive care. HERC average cost data are designed for research – the data provides a quick understanding of the average cost of VA health services. Resources for learning about the Inpatient Average Cost data are available on the HERC website. The VHA Labor Cost dataset can be used to determine the cost of staff time. For each type of personnel, the database gives the hourly labor costs from the MCA Office Account-Level Budgeter Cost Center (ALBCC) database and the Financial Management System (FMS). Data include the personnel type, total labor costs, workload, and hourly labor costs. The labor cost dataset is saved as an excel file in the Researcher’s Guide to Estimating VHA Labor Costs (VA intranet only). |
|||

|
Health Economics Resource Center (HERC) |
|
You have received this message because you are subscribed to VA Health Economics Resource Center. Access your Subscriber Preferences to make changes to your subscription or Unsubscribe. Get this as a forward? Sign Up to receive updates from HERC. Please do not reply as this email box is not monitored. To contact HERC please email herc@va.gov. |
||
 |