|
This
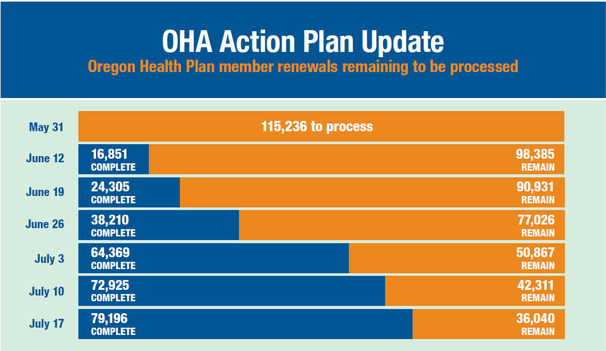
summer, a team of Oregon Health Authority staff and outside contractors are completing Medicaid eligibility renewals for approximately 115,000 cases
previously contained in the Cover Oregon database and other legacy systems. As of mid-July:
- Workers
had cleaned up more than 79,000 of the outstanding cases, putting OHA on track
to finish the work by the Aug. 31 deadline.
The painstaking work entails verifying whether an adult or
child who receives health coverage under Medicaid is still eligible to receive
it. OHA eligibility workers must manually transfer case files from outdated or
failed databases into the state’s new ONE system.
ONE allows Oregon Health Plan members to apply
for (and renew) benefits online. OHA and DHS are collaborating on a project to
centralize the application process for food stamps, temporary assistance,
Medicaid and other benefits in ONE.
Oregon’s
coordinated care organizations continue to advance health system transformation
by focusing on better care and better health outcomes while controlling health
care costs. That’s the takeaway from two recent reports on the performance and
stability of CCOs: the Oregon Health System Transformation Quarterly
Legislative report and the CCO Metrics report.
Highlights
of the CCO Metrics report show continued improvements in a number of key areas,
including:
-
Adolescent
well-care visits. CCOs continue to make large strides on this
measure, with 15 of 16 CCOs improving in 2016 and 13 achieving their individual
improvement target.
- Effective
contraceptive use among women at risk of unintended pregnancy. A new measure in 2015, the percentage of
women ages 18 - 50 who are using an effective contraceptive has increased 19
percent in two years.
- Developmental screening
in the first three years of life. CCOs continue to make large strides in the
percentage of children who are screened for risks of developmental, behavioral,
and social delays. In 2011, only 21 percent of young children received an
appropriate screening. Since then, the percentage has more than tripled to over
62 percent in 2016.
Read
both reports on our website.

The Behavioral Health Collaborative (BHC) has convened five
workgroups to further recommendations that will move the state’s behavioral
health system to a coordinated care model. The goals are to integrate
behavioral health with physical and oral health and to develop minimum
standards so all Oregonians receiving behavioral health services will have
consistency.
OHA convened the collaborative last summer. The 50-member
group includes representatives from peer support services, advocates, counties,
behavioral health providers, courts, DHS, CCOs, hospitals, education, law
enforcement and representatives from an Oregon Tribe and an urban Indian
organization.
The collaborative in March released the Behavioral Health
Collaborative Report, which
includes recommendations, and a mapping tool that displays interactive information about the state’s
behavioral health system.
The workgroups began meeting in May and will end in August.
The Governance and
Finance Workgroup, a workgroup of the Oregon Health Policy Board, is responsible
for:
- Developing guidelines for the development of a single-point of shared accountability;
- Developing
guidelines for approval of single plans of shared accountability;
- Identifying
the need for OAR (Oregon Administrative Rules) and contract changes; and
- Recommending
a financial incentive structure.
The Standards of Care
and Competencies Workgroup is facilitated through the Behavioral Health
Planner of the Addictions and Mental Health Planning and Advisory Council. This
group is responsible for:
- Establishing
core competencies;
- Recommending
minimum standards for care; and
- Recommending
mechanisms for co-management of individuals who require specialty behavioral
health care.
The Peer Delivered
Services Workgroup is a subcommittee of the Peer Delivered Services (PDS)
Core Team. This group is responsible for:
- Developing
standards, expectations, and monitoring guidelines for PDS;
- Recommending
a standardized training model; and
- Recommending
certification for peer supervisors.
The Workforce
Workgroup is facilitated through the Behavioral Health Planner of the
Addictions and Mental Health Planning and Advisory Council. This group is
responsible for recommending standards for a well-trained behavioral health
workforce.
The
Health Information Technology Oversight Council, a workgroup of the Oregon Health Policy Board,
is responsible for recommending how to use technology to integrate care across
the behavioral health system.

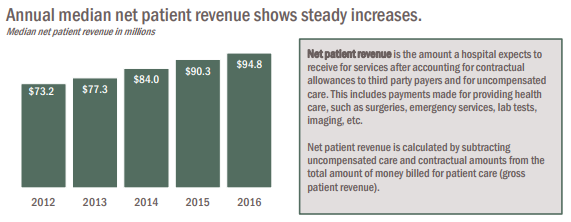
New reports show the financial
condition of Oregon hospitals in 2016, along with their performance
on key quality measures. According to these reports:
-
Overall margins for 2016 continue to remain
higher
than typically observed before the implementation of the Affordable Care Act
(ACA).
- Net patient revenue increased and charity care
remained low in
2016 after a sharp drop from 2013 to 2014.
- The fourth quarter of 2016 was
financially turbulent for hospitals with lower operating and total margins.
Overall, Oregon hospitals remain financially stable.
OHA requires 28 large “DRG” hospitals to submit data on 11 measures or “metrics” that include goals such as reducing health care-associated infections, reducing readmissions of patients after discharge, improving medication safety, improving overall patient experience, and screening for alcohol and substance use. In 2016, hospitals showed improvement on adverse drug events due to opioids, reduced central line-associated blood stream infections (CLABSI) and coordination on patient care with CCOs.
In addition, OHA released the Oregon Hospital Payment Report 2015. The report details the median amounts paid by commercial insurers for the most common inpatient and outpatient procedures that were performed in Oregon hospitals in 2015, as required by SB 900.
- Most procedures show sizable variations in paid amounts, both within and between hospitals.
- Among common outpatient procedures, heart electrophysiology studies were reported to have the highest median paid amount at $36,900.
- Among common inpatient procedures, heart valve replacement surgeries were reported to have the highest median paid amount at $84,700.
Reports from Washington, D.C. about Senate efforts to repeal
and replace the Affordable Care Act (ACA) remain fluid. Senate leaders indicate
they will vote early the week of Jul. 24. What proposals the Senate will vote
on remains uncertain.
This week, the Congressional Budget Office (CBO) scored a
Senate proposal to repeal the ACA, as well a modified version of the Better
Care Reconciliation Act (BCRA). According to the CBO, the repeal-only bill
would result in 32 million Americans losing health coverage by 2026. The
revised BCRA would result in 22 million Americans losing health coverage.
OHA and the Department of Consumer and Business
Services (DCBS) recently analyzed
the impact of BCRA on Oregon. Health policy experts and insurance
regulators found the Senate ACA “repeal and replace” proposal would:
-
Reduce health coverage: Result in 440,000 Oregonians losing health
coverage by 2025.
- Add costs to the State budget: Shift as much as $6.2 billion in costs from
the federal government to the state by 2026.
- Reduce jobs: Put as many as 35,000 health care jobs at risk
across Oregon.

Lori Coyner,
state Medicaid director, has left OHA. She plans to take some time off and explore new opportunities into health care. As state Medicaid director
for the past two years, Lori played a central role in Oregon’s ongoing
health transformation. She successfully led Oregon’s Section 1115 Medicaid
waiver renewal, oversaw the resetting of actuarially sound and federally approved
CCO rates, and played a major role in addressing recent OHP budget challenges.
Director Lynne Saxton said, "We’ll miss
Lori’s knowledge, energy and considerable skills." David Simnitt will step into
the role of interim state Medicaid director.
|
|