Pharmacologic Approaches to Glycemic Treatment
The American Diabetes Association (ADA) Standards of Care in Diabetes—2026, Pharmacologic Approaches to Glycemic Treatment, is the focus of this newsletter. The complete document offers insight into the treatment of all types of diabetes and includes sections on virtually every facet of diabetes management. At least half of the 17 sections of the standards of care are directly applicable to pharmacists in virtually any work setting. Readers are encouraged to download this document at no charge at ADA Guidelines 2026. Each section can be downloaded separately if desired.
Some changes for 2026
The 2026 ADA Standards of Care contains updates across key domains relevant to pharmacists. Pharmacologic therapy continues to evolve with expanded roles for certain incretin-based agents across glycemic control and comorbid conditions. There is also a greater emphasis on individualized treatment selection, shared decision making, addressing social determinants of health (SDOH) and reducing therapeutic inertia. Weight management is prioritized as a distinct treatment goal because of its multiplicity of beneficial effects. There is stronger guidance on structured lifestyle interventions and use of effective pharmacologic options. There is also increased recognition of metabolic dysfunction–associated liver disease (MASLD) and metabolic dysfunction–associated steatohepatitis (MASH) as important factors influencing medication choice, with therapies now targeting both glycemic and hepatic outcomes. Chronic kidney disease (CKD) management emphasizes earlier and combined use of kidney-protective agents and regular estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) testing. Broader cardiometabolic health updates highlight more aggressive risk factor control and the growing role of therapies that provide cardiovascular and heart failure benefits.
|
Glycemic Goals
|
A1C & Glucose Targets
|
CGM (Continuous Glucose Monitoring) Metrics
|
|
A1C (stringent): <6.5% Use if low hypoglycemia risk/recent diagnosis/otherwise healthy
|
Time in Range (70–180): >70% Best overall control metric
|
|
A1C (standard): <7% Default goal for most adults or <7.5% for some older healthy adults
|
Time <70 mg/dL: <4% Reduce hypoglycemia
|
|
A1C (less stringent): <8% for older/comorbid patients
|
Time <54 mg/dL: <1% Avoid dangerous lows
|
|
Pre-meal: 80–130 mg/dL Assess fasting trends
|
Time >180 mg/dL: <25% Limits hyperglycemia burden
|
|
Post-meal: <180 mg/dL Check 1–2 hrs after meals
|
|
Medication choices for type 2 diabetes
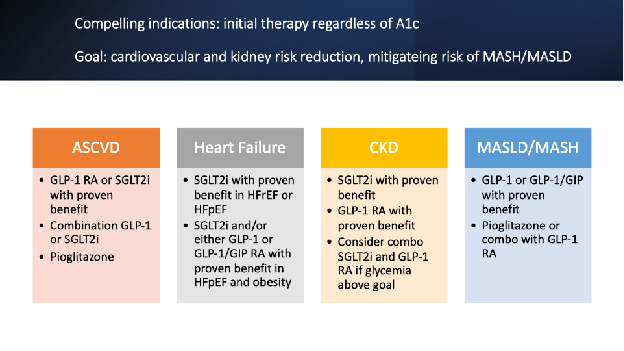
- The glycemic management of type 2 diabetes should include agents with proven cardiorenal effects in people with, or at high risk for atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), or chronic kidney disease (CKD) regardless of A1C levels.
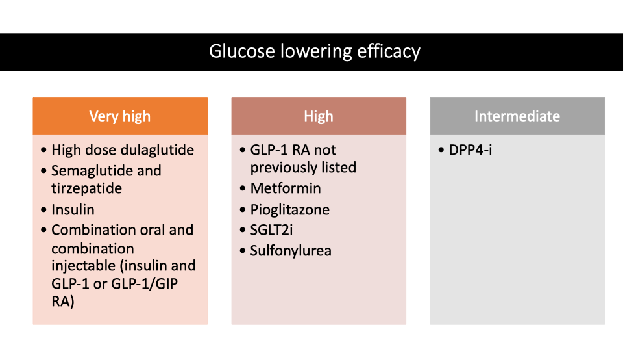
- Other agents for glycemic control should possess adequate efficacy to achieve goals, be less likely to cause hypoglycemia, and be helpful in weight management.
- Use a shared decision approach considering patient preference, cost, access, and risk of adverse effects.
Other key points
- In adults with type 2 diabetes without severe hyperglycemia or hyperglycemic crisis, glucagon-like peptide-1 (GLP-1) receptor agonists (RA) or dual glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonists should be the first injectable therapy.
- Continuous glucose monitoring (CGM) is recommended at diabetes onset for children, adolescents, and adults using insulin or therapies with hypoglycemia risk and at any time where CGM helps in management.
- Automated insulin delivery (AID) should be offered to all patients with type 1 as well as adults and children on multiple daily injections, continuous subcutaneous insulin infusion (CSII) or sensor augmented pumps and may also be helpful in type 2 patients on basal insulin.
- Healthy lifestyle, diabetes education and support, social determinants of health (SDOH), and avoidance of clinical inertia are essential components of diabetes management.
- GLP-1 based therapy can be used safely in dialysis to reduce cardiovascular risk.
- Monitor CKD using urine albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR) at onset and at least annually in type 2 and 5 years after diagnosis in type 1 diabetes.
- An angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) is strongly recommended for non-pregnant individuals with hypertension and CKD.
- The systolic blood pressure goal of under 120 mmHg should be encouraged for those at high cardiovascular or kidney risk.
- There are new recommendations for treatment of hyperglycemia in people undergoing cancer treatments, immunotherapy, or high dose glucocorticoid therapy.
  3MinuteExtraMile™: Take 3 minutes to:
- Identify the diabetes care and education specialists, dietitians, community health workers (especially in underserved communities), and diabetes education programs in your area and refer patients who are newly diagnosed or unable to reach goals.
- Help avoid clinical inertia by reminding patients that therapy may need to be revised if goals are not met after 3–6 months.
- Recommend vitamin B-12 monitoring or supplementation with metformin (low B-12 associated with neuropathy).
- Suggest glucagon for patients on insulin and provide hypoglycemia education.
- Review medications for guideline-directed therapy.
- Recognize social determinants of health (SDOH) factors that influence patient’s health status. Identify local resources that can offer assistance.
- Prioritize safety and avoid hypoglycemia, especially in older patients with comorbidities. Secretagogues and insulin are the primary offenders and there are options (incretin-based therapies and/or SGLT2i for instance) for decreasing doses or discontinuation.
James Bennett BsPharm, BCGP, CDCES
MT DPHHS Cardiovascular and Diabetes Programs consultant
Bozeman MT
For more information, contact: diabetes@mt.gov
1400 E Broadway
Helena, Montana 59620-2951
1-844-MTHLT4U (1-844-864-5848)
https://dphhs.mt.gov/publichealth/diabetes
|

