|
Diabetes & Kidney Health: What Pharmacists Need to Know for National Kidney Month

CKD occurs in 20-40% of people with diabetes and many of them are unaware of their condition. It is not unusual to discover CKD already present at diagnosis in type 2 diabetes.
CKD in the early stages is often asymptomatic and can go unnoticed until kidney damage has occurred. If left untreated, CKD can lead to progressive loss of kidney function ultimately resulting in dialysis or kidney transplant. Kidney damage in people with diabetes is associated with microvascular damage caused by elevated glucose and is complicated by the addition of hypertension, also common in people with type 2 diabetes.
The Centers for Disease Control (CDC) estimates for adults with CKD:
- 1 in 7 adults (14%) in the US have CKD.
- 9 out of 10 adults with CKD don’t know they have it.
- 1 out of 3 adults with severe CKD don’t know they have it.
People with diabetes and CKD have a markedly increased risk of cardiovascular disease. The American Diabetes Association (ADA) guidelines recommend optimizing glucose management and controlling blood pressure (goal Below 130/80) to prevent onset and/or worsening of kidney function, as well as the addition of pharmacological agents shown to have positive cardio-renal effects. Notably the ADA 2025 guidelines stress the use of maximally tolerated doses of an ACE or ARB in non-pregnant individuals with moderate to severely increased albuminuria to prevent worsening CKD and reduce cardiovascular events. ACE or ARB therapy is recommended for non-pregnant individuals with diabetes and hypertension with or without CKD.
|
Screening and testing for CKD
The two recommended tests are estimated glomerular filtration rate (eGFR), and urinary albumin to creatinine ratio (UACR). UACR testing is done using a “spot” urine sample to measure both creatinine and albumin. While eGFR testing rates are high, the UACR testing rates are suboptimal and highly variable within the medical community. A person is diagnosed with CKD by virtue of reduced eGFR and/or the presence of albuminuria therefore both tests are recommended at specific intervals. Both eGFR and UACR tests are essential because CKD can exist with normal eGFR but elevated albumin levels. Ensuring both tests are performed regularly improves early detection.
Recommendations for eGFR and UACR testing
- At least annually beginning 5 years after diagnosis with type 1, and at diagnosis with type 2 diabetes.
- In people with established CKD, monitor eGFR and UACR 1 to 4 times yearly.
-
CKD diagnostic criteria: eGFR < 60 ml/min per 1.73 m2 OR UACR 30 mg/g or higher

Managing CKD in people with type 2 diabetes
There are 4 classes of medications used to slow the decline in kidney function and reduce cardiovascular risk in people with diabetes and CKD. Among these, SGLT-2 inhibitors and GLP-1 Ras also help lower blood glucose while protecting kidney function.
- ACE or ARB
- SGLT-2 inhibitor
- Nonsteroidal mineralocorticoid receptor antagonist (finerenone).
- GLP-1 RA with proven benefit when needed to reach glycemic goal.
|
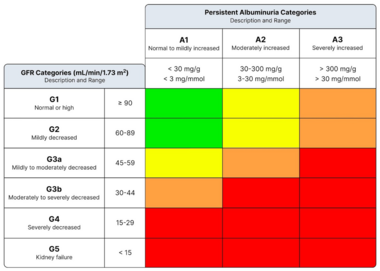
The 3MinuteExtraMile “save a kidney” encounter
The Heat Map: indicating level of risk for CKD progression and cardiovascular events.
Green: Low risk
Yellow: Moderately increased risk
Orange: High risk
Red: Very high risk
 References:
Resources for patients 2025
James Bennett BsPharm, BCGP, CDCES
MT DPH Cardiovascular and Diabetes Programs consultant
Bozeman MT
|
|
|
|

