|
Can a Supplement a Day Keep Asthma at Bay?
Regardless of practice setting, most pharmacists have experienced patients inquiring about the use of complementary and alternative methods (CAM) to help with a variety of health conditions. Although the use of CAM to treat respiratory conditions are not recommended by current asthma guidelines, patients may nonetheless ask about the potential safety and efficacy of a variety of supplements related to improving asthma symptoms.
Vitamin D has a large number of beneficial qualities, however, there is insufficient evidence to support its use for the adjunct treatment of asthma. Population research has noticed a correlation between low Vitamin D levels and increased asthma exacerbations, yet the clinical evidence is lacking on demonstrating a clear reduction in exacerbations or improvement in asthma symptoms.
Black Seed may be possibly effective for patients with asthma and COPD. This supplement has a variety of other names, including but not limited to, black caraway, black cumin, or fennel flower. Studies have shown mixed results with some demonstrating improved lung function and decreased wheezing/coughing after 3 months of use for patients with moderate-severe asthma who are already on conventional asthma medications. This supplement is considered likely safe for healthy adults when black seed oil is used orally at doses of up to 5 mL or 5 grams daily for up to 12 weeks. This supplement is generally well tolerated both orally and topically with the most common ADR being GI upset .
Maritime Pine may be possibly effective in patients with asthma who are on conventional asthma medications. Three small clinical trials compared the addition of standardized pine bark extract to those taking conventional treatment alone and found that there was a small increase in peak expiratory flow, decrease in asthma symptoms, and decreased use of rescue medications. In these studies a weight based dose of 1 mg/lb body weight or 100 mg daily was used. This supplement is considered possibly safe in healthy adults when used in doses of 50-450 mg daily for up to one year. Additionally, high doses (800 mg daily) have been used up to 16 days. Maritime pine is generally well tolerated with the most common ADRs being GI complaints, dizziness, and vertigo.
Patients may inquire about other supplements to help with asthma symptoms, however, there is insufficient evidence of any other products demonstrate a beneficial role in asthma care. As with any over the counter (OTC) supplement, it is important to educate patients that these products are not regulated by the FDA and that varying amounts of active ingredient may be present. USP products are verified by an independent third party to provide quality assurance regarding the contents of an OTC product. Always consider the patient’s medical history and current medications prior to recommending a supplement.
Summary of Effectiveness in Asthma Care
- Possibly effective as an adjunct treatment: Black seed and maritime pine
- Insufficient evidence: Vitamin D
- Unlikely effective: Oral or nebulized magnesium
Written by Jade Bosic-Reiniger, PharmD, MPH, BC-ADM, AE-C
De-intensifying Diabetes Medications
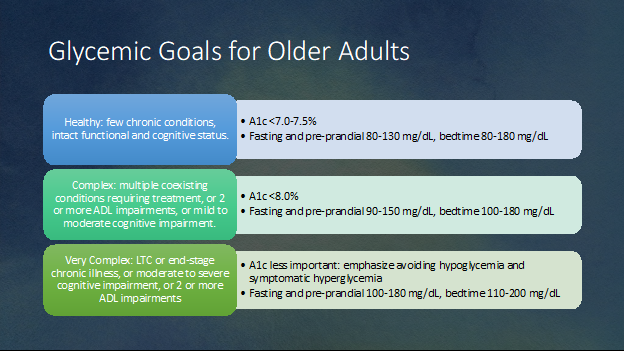
Our Diabetes Pharmacy Newsletters from March and April of this year reviewed the ADA 2023 guidelines for treatment of diabetes in older adults and can be accessed for more information on this subject. Adjusting treatment goals and medications with known hypoglycemia risk in older adults, particularly those with complex or poor health status is recommended. For that population, relaxing A1c and Time In Range targets and reducing or eliminating insulin and/or sulfonylureas should be attempted if possible while considering individualized patient goals. Despite evidence that the risk of emphasizing tight control and using hypoglycemia-related agents outweighs the benefits, many older adults remain on these therapies.
The National Physician Survey of Deintensifying Diabetes Medications for Older Adults With Type 2 Diabetes, asked physicians in general practice, geriatrics, and endocrinology what changes they would make in older patients taking medications associated with high risk of hypoglycemia. The questions were based on three scenarios where subjects were taking intermediate doses of hypoglycemia-inducing agents. Each scenario was approached several ways. For instance, in the “base case” the patient reported no hypoglycemia and no medication problems. Subsequently nine variations of each case were presented where patients reported such things as episodes of hypoglycemia or some issues with medication. In each variation the physicians were asked the same question: “what if any changes would you make in diabetes medications?” They were also asked what A1c goals they would set for patients in good, complex, and poor health categories.
Three scenarios:
- A 79-year-old woman in good health: A1c of 6.3% taking glimepiride.
- A 77-year-old man with multiple chronic conditions: A1c of 7.3% taking insulin glargine.
- A 77-year-old woman with advanced dementia: A1c of 7.7% taking glipizide.
Results of the survey:
The overall response rate from general medicine, geriatrics, and endocrinology was 37.5%. The reasons for deciding to change, reduce the dose, or discontinue a medication were varied, as was adjusting the target A1c to accommodate a person’s health status. It is interesting to see the differences in decision making based on practice setting described in the article as well as the attached reference relating to physician factors.
Conclusions:
- Most U.S. physicians would not deintensify or switch sulfonylureas or insulin for older adults with complex or poor health and higher A1c levels (7.3-7.7%).
- Most physicians targeted lower A1c levels than recommended for patients with complex and poor health and selecting a lower target was strongly associated with not deintensifying.
- Nearly all deintensified or changed therapy if a person reported recent hypoglycemia episodes.
 3MinuteExtraMile suggested action steps:
- Those of us involved in MTM services with Outcomes MTM are being paid to consult with patients and physicians about the use of sulfonylureas in older people. This is an opportunity to open the conversation about hypoglycemia symptoms, how they are monitoring blood sugar, and their target A1c.
- Think about both the person’s A1c or Time In Range target (if they know their numbers) and consider their health status. Is there a need to suggest relaxing glycemic goals?
- Deintensifying can include reducing a dose or discontinuing a medication. Discontinuing an offender and switching to a safer medication such as an SGLT2i, GLP-1 RA, or DPP-4i may be an option.
- Pharmacists in long term care often see type 2 patients in poor health being treated with complex insulin regimens, typically basal and sliding scale bolus insulin that puts the patient at high risk for hypoglycemia. Consider changing to more appropriate therapy.
- Resources:
Diabetes Medications Changes: Physician Factors
National Physician Survey
James Bennett BsPharm, BCGP, CDCES
Bozeman, MT
Please share with colleagues and encourage them to Click to subscribe
|


