|
We are excited to share this announcement! Even if you are not a Certified Asthma Educator please consider attending this conference.

Asthma and Smoking
Smoking is known to have negative impacts on lung function. Smoking causes bronchoconstriction which can be more significant in patients who already have worse lung function at baseline, such as people with asthma.
A study done in Spain and France compared: 1) people who never smoked, 2) current smokers and 3) former smokers. This showed current smokers experience greater prevalence of asthma and the atopic triad (asthma, eczema, and allergies), have worse Asthma Control Questionnaire (ACQ) scores, have more asthma exacerbations annually, have greater utilization of systemic corticosteroids, have poorer lung function, and decreased lung capacity.
Furthermore, in a systematic review of literature, it was found that smokers had higher incidence of asthma exacerbations, higher rates of life-threatening asthma attacks, and higher asthma related mortality when compared to people with asthma who did not smoke. Additionally, it was found that active and passive inhalation of cigarette smoke has negative impacts on asthma control. The figure below shows the systemic response to smoking in a patient with asthma.
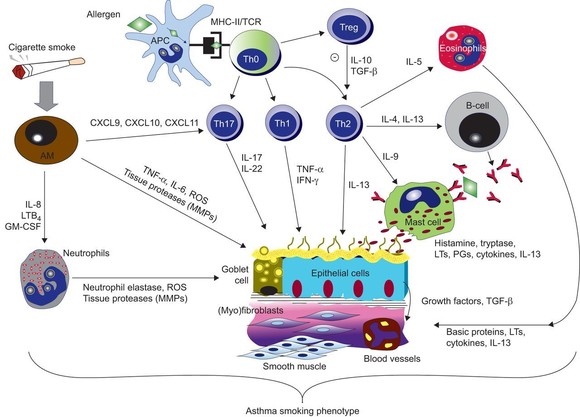
Image Source: Smoking and Asthma: Dangerous Liasons https://erj.ersjournals.com/content/41/3/716
Pharmacist Action Steps:
- Counsel patients on how smoking impacts asthma control and how it can lead to asthma exacerbations.
- Provide patient education on what smoking does to the lungs.
- Ask about tobacco use at every patient visit.
- Assess patients’ readiness to quit smoking.
- Offer information about the Montana Tobacco Quit Line including program benefits and offerings.
-
Educate patients on tobacco cessation products and help create a quitting plan.
- Follow up with the patient to provide resources and support throughout the quitting process and remember that quitting often requires multiple attempts.
Written by Cassidy Thompson, PharmD Candidate. Reviewed by Rachael Zins, PharmD, AE-C
ADA guidelines 2023: New Guidance on Cardiovascular Disease Management
The American Diabetes Association (ADA) has released its Standards of Care in Diabetes 2023 edition. This 2023 publication contains changes in several sections and supersedes all previous ADA guidelines and consensus statements.
Cardiovascular Disease and Risk Management:

ADA has changed its definition of hypertension and timing of treatment initiation to align with the 2017 American Heart Association/American College of Cardiology guidelines. Hypertension is defined as blood pressure at or above 130 mmHg systolic or 80 mmHg diastolic. Highlights are summarized below.
- Blood pressure should be measured at every office visit by a trained professional and hypertension diagnosis confirmed by two or more readings on two or more days.
- Those with elevated blood pressure (between 120 and 129 mmHg systolic and under 80 mmHg diastolic) should have the measurements confirmed on a seperate day.
- People with diabetes should be offered medication treatment if levels are at or above 130/80 mmHg.
- In pregnant patients with sustained blood pressure at or above 140/90 mmHg consider initiation of medication.
- All patients with diabetes should measure blood pressure at home.
|
Some changes were made in the recommendations for lipid management goals and treatments in people with and without atherosclerotic cardiovascular disease (ASCVD).
- People with diabetes aged 40-75 years with higher risk (i.e., one or more ASCVD risk factors) should be given a high intensity statin.
- The treatment target for higher risk individuals is a 50% reduction in LDL and a goal of under 70 mg/dL.
- Continue statin therapy in those over 75 years of age.
- Initiate moderate intensity statin therapy in those over 75 years of age.
- For those with established ASCVD initiate high intensity statin therapy with a goal of 50% reduction in LDL and a target of under 55 mg/dL
- Add ezetimibe or a PCSK9 inhibitor to maximally tolerated statin therapy if unable to reach goals.
Recommended Pharmacist Actions and Talking Points
- Clinicians are urged to do face-to-face goal setting. Encourage patients to know their goals and their current blood pressure and lipid levels
- Counsel people with diabetes about the importance of controlling blood pressure early on to avoid cardiovascular disease and microvascular complications. Mild blood pressure elevation often starts in the 30s and 40s and should not be ignored because it only gets worse. First line therapies, ACEs, ARBs, CCBs, and diuretics are well tolerated and inexpensive.
- Most adults with diabetes except during pregnancy should be taking a statin. A recent study indicated that statin therapy may make diabetes more difficult to control but that should not preclude the use of statins because of the positive benefit risk ratio. Advocate for statin initiation at the appropriate intensity for your patients with diabetes and insist that they know their numbers.
James Bennett BsPharm, BCGP, CDCES
Bozeman MT
Please share with colleagues and encourage them to Click to subscribe
|

