|
We're growing and changing our content! In order to share a broader pharmacy-based message, this newsletter will now include content for asthma, diabetes, and cardiovascular health. Written and edited by Pharmacists and Pharmacy Students, we'll continue to strive to provide high-level, accurate content to help you care for our Montana communities.
Asthma
Whether your day is spent on trails, the water with a fly rod in hand, or at home, a summer day in Big Sky Country is tough to beat. Summer and fall in Montana can also bring wildfires and clouds of smoke that blotch out the sky. Smoke is a huge trigger for people with lung diseases such as asthma and COPD. This article will discuss guidelines-based asthma care and what to do if your patient’s asthma suddenly becomes uncontrolled.
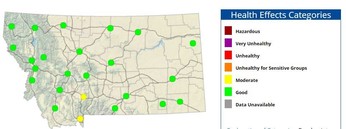
Remind patents to check the air quality in their area before heading outside. Todaysair.mt.gov, from the Montana Department of Environmental Quality, has an interactive map that allows users to see hourly ambient air quality conditions in their area. Air quality is typically measured in PM2.5. What is PM2.5? PM2.5 stands for particle matter that is fine enough, less than or equal to 2.5 micrometers, to be inhaled.2 Under the Clean Air Act, the EPA, sets and reviews national air quality standards. Measurements are taken across the United States to collect data which is then distributed to local agencies to protect public health and the environment.
|
What steps can be taken to avoid the smoke?
Sometimes the simplest recommendations are the hardest to follow: stay inside. For most people, staying inside the entire summer is not an option. Here are a few pro-tips to get your patients through the haze:
- Avoid strenuous outdoor activities
- Limit the amount of time spent outside
- Consider moving physical activities inside or rescheduling them
- ALWAYS carry a rescue inhaler
- Refill your asthma medications before the smoke becomes an issue
- Protect your indoor air quality by limiting air pollutants in the home
 |
|
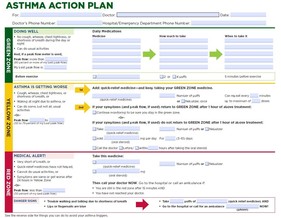
If your patients have asthma and have not received an asthma action plan, make sure they talk to their provider right away. Asthma action plans are individualized guides that show patients and their caregivers the steps needed for preventing asthma attacks and managing worsening symptoms. There is also guidance on when to call the provider or 911. Here is one version of an asthma action plan. |
ATTENTION PHARMACISTS: Keep an eye out for patients filling inhalers during the smoky season. If you notice a patient picking up a rescue inhaler more frequently, this is a great opportunity to have a 1-on-1 discussion with them. This would also be an excellent time to ask about inhaler technique and complete an Asthma Control Test (ACT). The ACT is a validated 5-question questionnaire that evaluates asthma control. If appropriate, consider speaking with the patient’s provider about stepping up the patient’s medication according to the EPR-3 Guidelines for the Diagnosis and Management of Asthma.
Authors: Shelby Brooks, PharmD Candidate, Kyle Van Eimerem, PharmD Candidate, Rachael Zins, PharmD, AE-C
Diabetes
Statins And People With Diabetes
People with diabetes between the ages of 40 and 75 years of age should receive statin therapy.
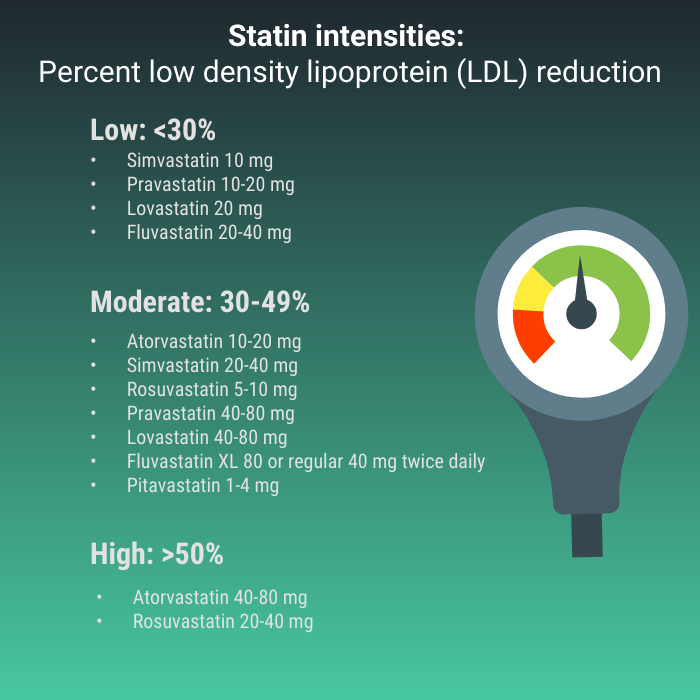
The goal of statin therapy is to reduce atherosclerotic cardiovascular disease (ASCVD), defined as coronary heart disease, cerebrovascular disease, or peripheral arterial disease. In this 40–75 year-old age group, moderate intensity statin therapy can reduce ASCVD events by 25%. People over the age of 75 may also benefit from statin therapy because cardiovascular risk increases with age. Younger adults aged 20-39 years who have additional (ASCVD) risk factors may also benefit from statin therapy. Statin intensities for people with diabetes start with moderate-intensity or high-intensity. Low-intensity is reserved for people unable to tolerate the recommended intensity
 Centers for Disease Control (CDC) diabetes statistics 2020
- 43.5% have reached target lipid goals of non-HDL levels under 130 mg/dL
- 58.4% of people between the ages of 40 and 75 are receiving statin therapy
- Risk of death at an early age 60% higher for adults with diabetes
The ADA, the American Heart Association/American College of Cardiology (AHA/ACC), and the American Association of Clinical Endocrinologists/American College of Endocrinology (AACE/ACE) have lipid management guidelines. Non-high-density cholesterol (non-HDL) level is included in goal setting because of the type 2 diabetes triad of elevated LDL and triglycerides, and low HDL.
Guidelines and goals:
ADA and AHA/ACC have similar goals and strategies whereas AACE/ACE has an additional “Extreme Risk” category. All include lifestyle intervention.
AACE/ACE:
- High risk (diabetes and no other risk factors): LDL < 70 mg/dL and non-HDL < 130 mg/dL: Moderate intensity statin
- Very high risk (diabetes with one or more extra risk factors): LDL < 70 mg/dL and non-HDL < 100 mg/dL: High intensity statin
- Extreme risk (diabetes with established clinical ASCVD): LDL < 55 mg/dL and non-HDL < 80 mg/dL: High intensity statin
ADA and AHA/ACC (similar guidelines):
- Adults ages 40-75 years and no ASCVD: Moderate intensity statin and lifestyle intervention. For this age group at higher risk, a high-intensity statin may be used.
- Adults ages 20-39 years and additional ASCVD risk factors: moderate-intensity statin or high-intensity if at higher risk.
- Adults of all ages with clinical ASCVD: high intensity statin.
- The LDL goal is to reach the percent reduction aligning with the statin intensity. For high-risk patients with LDL of above 70 mg/dL on maximally tolerated statin, consider add on therapy.
What can pharmacists do?
-
Ensure that patients with diabetes, recommended for statin therapy, are taking such therapy at the appropriate intensity.
-
Offer solutions to perceived statin intolerance, such as alternate day dosing, reducing daily dosage, or changing statins. Look for drug interactions that increase statin exposure.
-
Stress cardiovascular risk reduction rather than cholesterol reduction. For example, a 1% reduction in LDL produces about a 1% reduction in risk for ASCVD. Statin therapy can produce a 25% reduction in ASCVD events.
-
Talk about the reasons for statin hesitancy and risk/benefit. Combat misinformation.
James Bennett BsPharm, CDCES, BCGP
Bozeman MT
References for Asthma content:
1. Montana Department of Environmental Quality. (2021). Wildfire smoke outlook. Retrieved from: https://svc.mt.gov/deq/todaysair/
2. Guidelines for the Diagnosis and Management of Asthma 2007 (EPR-3). National Heart, Lung and Blood institute website. Accessed July 15, 2021. https://www
3. Air trends (5/21/21). United States Environmental Protection Agencie website. Accessed July 15, 2021. https://www.epa.gov/air-trends/particulate-matter-pm25-trends/.
4. Asthma (4/28/21). PrimeWest Health website. Accessed July 15, 2021. https://www.primewest.org/asthma/.
5. Welcome to the Asthma Control Test (5/1/21). GlaxoSmithKline website. Accessed July 15, 2021. https://www.asthmacontroltest.com/en-gb/welcome/.
6. 2021 GINA MAIN REPORT. Global Initiative for Asthma website. Accessed July 15, 2021. https://ginasthma.org/gina-reports/.
7. Guidelines for the Diagnosis and Management of Asthma 2007 (EPR-3). National Heart, Lung and Blood institute website. Accessed July 15, 2021. https://www.nhlbi.nih.gov/health-topics/guidelines-for-diagnosis-management-of-asthma/.
References for Diabetes:
ACC/AHA 2018 Guideline on Management of Blood Cholesterol
Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2021
Cholesterol Lowering Drugs, K. Feingold MD ncbi.nim.nih.gov
Centers for Disease Control Diabetes Statistics 2020
Please share with colleagues and encourage them to Click to subscribe
|

