Under-prescribing of recommended therapies:
Can pharmacists influence guideline-directed diabetes care?
Our past newsletters have addressed the American Diabetes Association (ADA) Guidelines as they pertain to certain drug classes, and the rationale behind the available choices. Members of the sodium glucose transporter 2 inhibitors (SGLT-2 inhibitors) and the glucagon-like peptide receptor agonists (GLP-1 RA) are receiving attention because of their use in compelling indications to treat diabetes comorbidities. They have moved up in the treatment hierarchy to the place where they can be first line choices along with metformin and lifestyle intervention. Some of the SGLT-2 inhibitors may be used for people without diabetes in the treatment of heart failure and chronic kidney disease.
Although the guidelines are clear on the use of SGLT-2 inhibitors, according to a recent study by Jeong et al*, two thirds of the patients meeting the criteria for SGLT-2 inhibitor therapy are not having them prescribed. The American Heart Association, American Diabetes Association, KIDIGO (Kidney Disease: Improving Global Outcomes), and others have voiced the opinion that these therapies are underutilized.
Focus on the SGLT-2 inhibitors:
SGLT-2 inhibitors are indicated in the treatment of type 2 diabetes.
As monotherapy they can lower A1c by .5% to 1%.
Long-term Cardiovascular Outcome Trials (CVOT) to assess the safety of new type 2 diabetes drug introductions were mandated by the Food and Drug Administration in 2008. Information about these trials, cardiovascular safety, and cardio-renal trials are frequently updated in the ADA “Living Standards of Care” the latest update occurred June of 2021.
Note: that these studies are not identical in design for each drug. For instance, they may have different primary and secondary end points, exclusion criteria, etc., so universal application of the results of one study to all drugs in a class is not recommended.
|
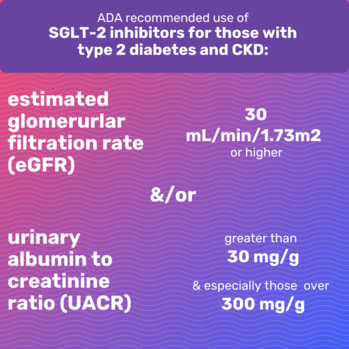
ADA Recommendations: Kidney disease and heart failure
 |
|
Current evidence demonstrates that rates of hospitalization for heart failure are twice as high for people with diabetes compared to those without and that rates have improved in recent trials with SGLT-2 inhibitors. Therefore, in patients with established heart failure with reduced ejection fraction (HFrEF) an SGLT-2 with proven benefit is recommended to reduce worsening heart failure and cardiovascular death. |
Current indications for specific agents marketed in the United States
Although there are experts who believe the SGLT-2 inhibitor cardio-renal effects are a class phenomenon, the Food and Drug Administration has only allowed manufacturers to state indications based on specific study data.
-
Dapagliflozin (Farxiga)**: To improve glycemic control in type 2 diabetes, to reduce risk of sustained eGFR decline, end stage renal disease, cardiovascular death, and hospitalization for heart failure (HFrEF) in adults with CKD. In type 2 diabetes to reduce risk of heart failure-related hospitalization in patients with established cardiovascular disease or multiple cardiovascular risk factors
-
Canagliflozin (Invokana)**: To improve glycemic control in type 2 diabetes, in type 2 patients with established cardiovascular disease to reduce cardiovascular events, to reduce kidney disease progression, cardiovascular related risk and hospitalization for heart failure in type 2 patients with nephropathy and albuminuria > 300 mg/day
-
Empagliflozin (Jardiance)**: To improve glycemic control in type 2 diabetes, to reduce the risk of cardiovascular death in type 2 patients with established cardiovascular disease.
-
Ertugliflozin (Steglatro)**: To improve glycemic control in type 2 diabetes
Discussion for pharmacists
Even in patients with or at risk for CKD and who have A1c levels near target, the use of SGLT-2 inhibitors may be indicated. There may be clinical inertia involved in the failure to prescribe these drugs to people whose diabetes is in control but whose kidney function or heart failure treatment is inadequate. It is postulated that primary care providers may be reluctant to prescribe these medications and instead refer to cardiologists, nephrologists, or endocrinologists. Patient out of pocket cost is always a factor to be considered so choices of a particular agent may be limited.
-
Identify patients with diabetes by reviewing charts and looking for therapies that indicate treatment for heart failure or a prior cardiovascular event.
-
Ask diabetes patients about their kidney function tests i.e., have they been diagnosed with reduced kidney function and if so, do they know the numbers such as what CKD stage they are in or their eGFR.
-
Develop your own talking points or “3-minute elevator speech” to quickly inform patients about a beneficial therapy and suggest that they talk to the provider at their next visit.
-
Get familiar with the patient counselling points for SGLT-2 inhibitors such as maintaining adequate fluid intake and monitoring for genital mycotic and urinary tract infections.
Final thoughts
Pharmacists in almost any practice setting can help patients by staying up to date on the latest therapies and being proactive in referring patients. These days patients can be their own best advocates in the provider’s office. If there is a therapy that has potential and is recommended in the disease state guidelines, patients can be confident in asking their provider to make the assessment.
James Bennett RPh, BCGP, CDCES
Bozeman MT 59715
*Jeong SJ, Lee SE, Shin DH, et al. Barriers to initiating SGLT2 inhibitors in diabetic kidney disease: a real-world study. BMC Nephrol. 2021;22:177. doi:10.1186/s12882-021-02381-3
**manufacturer prescribing information
ADA: American Diabetes Association
SGLT-2i or SGLT-2 inhibitor: Sodium glucose co-transporter 2 inhibitor
HFrEF: heart failure with reduced ejection fraction
CKD: chronic kidney disease
DKD: diabetic kidney disease
Encourage patients with diabetes to visit a Montana Diabetes Care and Education Specialist (DCES). If one is not located in your area, telehealth services may be available for patients to use, instead.
Please share with colleagues and encourage them to Click to subscribe
|

